Tafluprost (formerly MK-2452; MK2452; AFP-168; Taflotan; Zioptan) is a prostaglandin (PG) analog used as an anti-glaucoma drug. Tafluprost is applied topically (as eye drops) to treat ocular hypertension and regulate the advancement of glaucoma. It lowers intraocular pressure by causing the eyes to expel more aqueous fluid.
Physicochemical Properties
| Molecular Formula | C25H34F2O5 |
| Molecular Weight | 452.5313 |
| Exact Mass | 452.237 |
| Elemental Analysis | C, 66.35; H, 7.57; F, 8.40; O, 17.68 |
| CAS # | 209860-87-7 |
| Related CAS # | 209860-88-8 (Tafluprost acid); 157283-68-6 (Travoprost) |
| PubChem CID | 9868491 |
| Appearance | Colorless to light yellow liquid |
| Density | 1.2±0.1 g/cm3 |
| Boiling Point | 552.9±50.0 °C at 760 mmHg |
| Flash Point | 288.2±30.1 °C |
| Vapour Pressure | 0.0±1.6 mmHg at 25°C |
| Index of Refraction | 1.549 |
| LogP | 4.23 |
| Hydrogen Bond Donor Count | 2 |
| Hydrogen Bond Acceptor Count | 7 |
| Rotatable Bond Count | 13 |
| Heavy Atom Count | 32 |
| Complexity | 614 |
| Defined Atom Stereocenter Count | 4 |
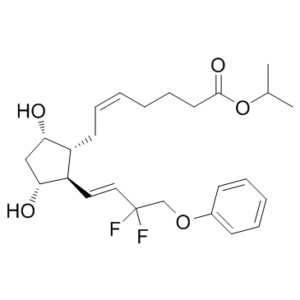
| SMILES | FC(C([H])([H])OC1C([H])=C([H])C([H])=C([H])C=1[H])(/C(/[H])=C(\[H])/[C@@]1([H])[C@@]([H])(C([H])([H])[C@@]([H])([C@]1([H])C([H])([H])C([H])=C([H])C([H])([H])C([H])([H])C([H])([H])C(=O)OC([H])(C([H])([H])[H])C([H])([H])[H])O[H])O[H])F |
| InChi Key | WSNODXPBBALQOF-VEJSHDCNSA-N |
| InChi Code | InChI=1S/C25H34F2O5/c1-18(2)32-24(30)13-9-4-3-8-12-20-21(23(29)16-22(20)28)14-15-25(26,27)17-31-19-10-6-5-7-11-19/h3,5-8,10-11,14-15,18,20-23,28-29H,4,9,12-13,16-17H2,1-2H3/b8-3-,15-14+/t20-,21-,22+,23-/m1/s1 |
| Chemical Name | propan-2-yl (Z)-7-[(1R,2R,3R,5S)-2-[(E)-3,3-difluoro-4-phenoxybut-1-enyl]-3,5-dihydroxycyclopentyl]hept-5-enoate |
| Synonyms | AFP-168; MK2452; AFP-168; MK-2452; Tafluprost; 209860-87-7; Saflutan; 1O6WQ6T7G3; AFP-168; MK 2452; Saflutan; Taflotan; Tapros; Zioptan |
| HS Tariff Code | 2934.99.9001 |
| Storage |
Powder-20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month |
| Shipping Condition | Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs) |
Biological Activity
| Targets | PGF2α |
| ln Vitro | Tafluprost (3 μM, 48 h) causes RGC-5 cells to produce fewer cells[1]. Tafluprost (0.1-100 μM, 48 h) increases RGC-5 cell viability in a dose-dependent way[2]. |
| ln Vivo | Tafluprost (0.0015% AFP168 eye drops, used for 14 days) as a makeup Sprague-Dawley can decrease nerve cell apoptosis, raise RGC cell vitality, and lower intraocular pressure caused by optic nerve compression (ONC)[2]. |
| Cell Assay |
Cell Line: RGC Concentration: 0.1, 1, 3, 10, 100 μM Incubation Time: 48 h Result: Enhanced the viability of these cells in a dose-dependent fashion, with an optimal concentration of 3μM. Increased the relative fluorescence intensity (RFI). |
| Animal Protocol |
Male Sprague rat model 0.0015% Via eye drops C57BL/6J, and EP1, EP2, EP3 and postaglandin F (FP) receptor-deficient wild-type (WT), EP1KO, EP2KO, EP3KO and FPKO, respectively mice were bred and acclimatised under a 12-h (6:00-18:00) light-dark cycle. To evaluate effects of tafluprost (0.002%) on IOP at night, a single 3 microl drop of tafluprost solution was applied topically at 18:00 once into one eye in each mouse. IOP was measured 3 h after the application with a microneedle method. To clarify whether endogenous prostaglandin is concerned with the tafluprost-induced IOP reduction, we applied 0.1% diclofenac Na, a cyclo-oxygenase inhibitor or PBS 30 min before the application of tafluprost in WT and EP3KO mice and measured IOP 3 h after the tafluprost application. We also determined whether animals responded predictably to 0.1% bunazosin HCl, a drug known to increase uveoscleral outflow. Results: 3 h after the application of 0.0015% tafluprost, mean (SEM) IOP reductions were 25.8 (2.1)% 26.3 (0.8)% 24.2 (1.4)% 16.5 (1.7)% and -0.9 (1.5)% in WT, EP1KO, EP2KO, EP3KO and FPKO mice, respectively. IOP reductions in EP3KO and FPKO mice were significantly smaller than in WT mice. Pretreatment with diclofenac Na significantly attenuated the IOP lowering effect of tafluprost in WT mice but not in EP3KO mice. Bunazosin HCl lowered IOP significantly in all genotypes by the same amount.[3] This clinical study included 28 glaucoma patients (28 eyes) with a treatment history of latanoprost ophthalmic solution (Xalatan(®)) or travoprost ophthalmic solution (Travatan Z(®)), who presented with corneal epithelial disorders. The subjects were switched to BAK-reduced tafluprost, and its effect on the ocular surface was examined after 1 and 2 months of treatment [using fluorescein staining score, hyperemia, tear film breakup time, and intraocular pressure (IOP) lowering]. Results: In all analyzed subjects (N=27), the fluorescein staining score was significantly improved after switching to BAK-reduced tafluprost (P<0.0001). Conversely, the IOP-lowering effect was not notably changed. The subjects switched from latanoprost (n=10) showed significant improvement in fluorescein staining score (P<0.05) as well as in IOP lowering (P<0.01). The subjects switched from travoprost (n=17) also showed significant improvement in fluorescein staining score (P<0.001), but without a significant change in IOP lowering. Conclusions: Tafluprost with reduced BAK has potential as a superior antiglaucoma drug, not only for its IOP-lowering effect, but also for its good corneal safety profile.[4] |
| ADME/Pharmacokinetics |
Absorption, Distribution and Excretion Following instillation, tafluprost is absorbed through the cornea and is hydrolyzed to the biologically active acid metabolite, tafluprost acid. Tafluprost is an ester which makes the drug lipophillic enough to be quickly absorbed through. When administered to the eye, the peak plasma concentration (Cmax) and time to peak plasma concentration (Tmax) of tafluprost acid in healthy subjects was 26 pg/mL and 10 minutes respectively. a AUC, tafluprost acid = 394 pg*min/mL - 432 pg*min/mL. Mean plasma tafluprost acid concentrations were below the limit of quantification of the bioanalytical assay (10 pg/mL) at 30 minutes following topical ocular administration of tafluprost 0.0015% ophthalmic solution. In male rats, it was observed that tafluprost was excreted into the feces. The highest concentration of tafluprost acid was found in the cornea and conjunctiva. Metabolism / Metabolites Tafluprost is an ester prodrug which is rapidly hydrolyzed by corneal esterases to form its biologically active acid metabolite. Tafluprost acid is further metabolized via fatty acid β-oxidation and phase II conjugation into 1,2,3,4-tetranor acid. |
| Toxicity/Toxicokinetics |
Effects During Pregnancy and Lactation ◉ Summary of Use during Lactation No information is available on the use of tafluprost during breastfeeding. Because of the extremely low levels in plasma after application to the eye, it is not likely to reach the breastmilk or bloodstream of the infant or to cause any adverse effects in breastfed infants. Professional guidelines consider prostaglandin eye drops acceptable during breastfeeding. To further diminish the amount of drug that reaches the breastmilk after using eye drops, place pressure over the tear duct by the corner of the eye for 1 minute or more, then remove the excess solution with an absorbent tissue. ◉ Effects in Breastfed Infants Relevant published information was not found as of the revision date. ◉ Effects on Lactation and Breastmilk Relevant published information was not found as of the revision date. |
| References |
[1]. Prospective observational post-marketing study of tafluprost for glaucoma and ocular hypertension: short-term efficacy and safety. Adv Ther, 2014. 31(4): p. 461-71. [2]. Tafluprost protects rat retinal ganglion cells from apoptosis in vitro and in vivo. Graefes Arch Clin Exp Ophthalmol. 2009 Oct;247(10):1353-60. [3]. The IOP-lowering effects and mechanism of action of tafluprost in prostanoid receptor-deficient mice. Br J Ophthalmol. 2007 May;91(5):673-6. [4]. Comparison of corneal safety and intraocular pressure-lowering effect of tafluprost ophthalmic solution with other prostaglandin ophthalmic solutions. J Ocul Pharmacol Ther, 2014. 30(4): p. 340-5. [5]. Effects of tafluprost treatment for 3 years in patients with normal-tension glaucoma. Clin Ophthalmol, 2013. 7: p. 1411-6. |
| Additional Infomation |
Tafluprost is a prostaglandin Falpha that is prostaglandin F2alpha in which the carboxylic acid function has been converted to the corresponding isopropyl ester and the 3-hydroxy-1-octenyl side-chain is substituted by 3,3-difluoro-4-phenoxybut-1-enyl. Used for treatment of elevated intraocular pressure in patients with open-angle glaucoma or ocular hypertension. It has a role as a prostaglandin receptor agonist. It is a prostaglandins Falpha, an organofluorine compound and an isopropyl ester. It is functionally related to a prostaglandin F2alpha. A prostaglandin analogue ester prodrug used topically (as eye drops) to control the progression of glaucoma and in the management of ocular hypertension. Chemically, tafluprost is a fluorinated analog of prostaglandin F2-alpha. Tafluprost was approved for use in the U.S. on February 10, 2012. Tafluprost is a Prostaglandin Analog. The mechanism of action of tafluprost is as a Prostaglandin Receptor Agonist. The physiologic effect of tafluprost is by means of Increased Prostaglandin Activity. Drug Indication Tafluprost is indicated for reducing elevated intraocular pressure in patients with open-angle glaucoma or ocular hypertension. FDA Label Treatment of glaucoma Mechanism of Action Tafluprost acid is a prostanoid selective FP receptor agonist that is believed to reduce the intraocular pressure (IOP) by increasing the outflow of aqueous humor. Studies in animals and humans suggest that the main mechanism of action is increased uveoscleral outflow. This study investigated the intraocular pressure (IOP)-lowering effects and safety of tafluprost ophthalmic solution 0.0015% in actual clinical practice. Methods: We started a mandatory prospective 2-year observational study, which collected IOP, conjunctival hyperemia score, corneal staining score, and adverse event data from glaucoma and ocular hypertension (OH) patients not previously treated with tafluprost at 2, 12, and 24 months. This report analyzes the 2-month findings. Results: Of the 4,180 patients from 553 medical institutions in Japan, most patients had primary open-angle glaucoma (POAG, 38.1%) or normal-tension glaucoma (NTG, 44.2%). After 2 months of tafluprost administration, IOP was significantly reduced by 4.3 ± 5.2 mmHg in POAG, 2.4 ± 2.5 mmHg in NTG, 3.6 ± 5.3 mmHg in primary angle-closure glaucoma, 5.6 ± 7.1 mmHg in other types of glaucoma, and 5.3 ± 4.8 mmHg in OH. IOP was significantly reduced by 4.3 ± 4.0 mmHg in the naïve monotherapy group, 1.9 ± 3.5 mmHg in switching from prior treatment, and 3.7 ± 4.1 mmHg in the add-on therapy group. Among patients switched, the prostaglandin analog (PGA) latanoprost was the previous predominant drug (57.4%), followed by travoprost (13.8%). Significant IOP reductions were observed by 1.5 ± 3.4 mmHg in switching from latanoprost and 1.3 ± 3.7 mmHg in switching from travoprost. The conjunctival hyperemia score peaked at 1 month in the naïve monotherapy and add-on therapy groups, whereas it was significantly decreased in patients switched from another PGA. The corneal staining score showed no particular changes. Incidence of adverse drug reaction (ADR) was 7.70 % (322/4,180 patients), and all major ADRs involved the eyes or skin around the eyes. Conclusion: Tafluprost showed significant IOP-lowering effects without any safety concerns in patients with various types of glaucoma and OH in daily clinical practice and tafluprost is highly effective in any therapeutic patterns.[1] Background: To investigate whether tafluprost, which is a prostaglandin-related compound and an anti-glaucoma drug, has a direct anti-apoptotic effect in cultured retinal ganglion cells (RGCs) and rat RGCs in retinas with optic nerve crush (ONC). Methods: RGC-5 cells were induced to undergo apoptosis by a serum deprivation and by exogenous glutamate. The level of cell death with or without tafluprost was monitored by an XTT assay and by immunocytochemistry with activated caspase-3. Changes in intracellular calcium ([Ca(2+)]i) levels were measured with fluo-4 fluorescence. Rat RGCs were degenerated by ONC. After topical instillation of tafluprost for 7 and 14 days, the numbers of retrograde-labeled RGCs were counted. Retinal flatmounts were subjected to terminal dUTP nick end labeling (TUNEL) staining to detect apoptotic cells. Results: Tafluprost dose-dependently promoted RGC-5 cell viability with an optimum concentration of 3 microM (p = 0.006). Tafluprost significantly reduced caspase-3-positive cells and suppressed [Ca(+2)]i evoked by exogenous glutamate. The cGMP-dependent protein kinase inhibitor and KT-5823 partially blocked the rescue effect of tafluprost (p = 0.002). The survival rate of RGCs significantly increased in eyes treated with tafluprost (p = 0.01), and the prevalence of TUNEL-positive cells was significantly decreased 14 days after ONC (p < 0.001). Conclusions: These data suggest that tafluprost has an anti-apoptotic effect in RGCs.[2] |
Solubility Data
| Solubility (In Vitro) | DMSO: ≥ 270 mg/mL (~596.7 mM) |
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 2.25 mg/mL (4.97 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 22.5 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 2.25 mg/mL (4.97 mM) (saturation unknown) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 22.5 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. Solubility in Formulation 3: ≥ 2.25 mg/mL (4.97 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 22.5 mg/mL clear DMSO stock solution to 900 μL of corn oil and mix evenly. (Please use freshly prepared in vivo formulations for optimal results.) |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 2.2098 mL | 11.0490 mL | 22.0980 mL | |
| 5 mM | 0.4420 mL | 2.2098 mL | 4.4196 mL | |
| 10 mM | 0.2210 mL | 1.1049 mL | 2.2098 mL |