Metoprolol Succinate (Toprol XL)is a potent and cardioselective β1 receptor blocker medication, which is used to treat hypertension and heart failure. In the left ventricular (LV) myocardium of dogs suffering from heart failure (HF), metoprolol reduces the rate of cardiomyocyte apoptosis. Heart failure (HF) is not necessary for metoprolol to induce the expression of Bcl-2, which in and of itself provides protection.
Physicochemical Properties
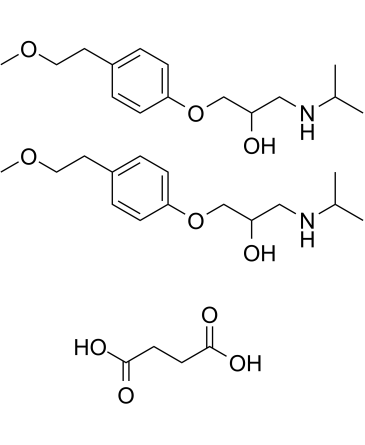
| Molecular Formula | C34H56N2O10 |
| Molecular Weight | 652.8159 |
| Exact Mass | 652.393 |
| Elemental Analysis | C, 62.55; H, 8.65; N, 4.29; O, 24.51 |
| CAS # | 98418-47-4 |
| Related CAS # | Metoprolol succinate;98418-47-4;Metoprolol-d7 hydrochloride;1219798-61-4;Metoprolol tartrate;56392-17-7;Metoprolol-d7;959787-96-3;(R)-Metoprolol-d7;1292907-84-6;(S)-Metoprolol-d7;1292906-91-2;Metoprolol-d5;959786-79-9; 51384-51-1; 56392-18-8 (HCl); 80274-67-5 (fumarate); 98418-47-4 (succinate) |
| PubChem CID | 62937 |
| Appearance | White to off-white solid powder |
| Boiling Point | 398.6ºC at 760 mmHg |
| Flash Point | 194.9ºC |
| LogP | 3.944 |
| Hydrogen Bond Donor Count | 6 |
| Hydrogen Bond Acceptor Count | 12 |
| Rotatable Bond Count | 21 |
| Heavy Atom Count | 46 |
| Complexity | 308 |
| Defined Atom Stereocenter Count | 0 |
| SMILES | O(C1C([H])=C([H])C(=C([H])C=1[H])C([H])([H])C([H])([H])OC([H])([H])[H])C([H])([H])C([H])(C([H])([H])N([H])C([H])(C([H])([H])[H])C([H])([H])[H])O[H].O(C1C([H])=C([H])C(=C([H])C=1[H])C([H])([H])C([H])([H])OC([H])([H])[H])C([H])([H])C([H])(C([H])([H])N([H])C([H])(C([H])([H])[H])C([H])([H])[H])O[H].O([H])C(C([H])([H])C([H])([H])C(=O)O[H])=O |
| InChi Key | RGHAZVBIOOEVQX-UHFFFAOYSA-N |
| InChi Code | InChI=1S/2C15H25NO3.C4H6O4/c2*1-12(2)16-10-14(17)11-19-15-6-4-13(5-7-15)8-9-18-3;5-3(6)1-2-4(7)8/h2*4-7,12,14,16-17H,8-11H2,1-3H3;1-2H2,(H,5,6)(H,7,8) |
| Chemical Name | butanedioic acid;1-[4-(2-methoxyethyl)phenoxy]-3-(propan-2-ylamino)propan-2-ol |
| Synonyms | Metoprolol succinate; Dutoprol; Selozok; Toprol XL; Seloken-ZOK; H 93/26 succinate; Spesicor Dos; H 93/26 succinate; Toprol |
| HS Tariff Code | 2934.99.9001 |
| Storage |
Powder-20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month Note: Please store this product in a sealed and protected environment, avoid exposure to moisture. |
| Shipping Condition | Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs) |
Biological Activity
| Targets | β1 adrenoceptor |
| ln Vitro | Metoprolol (0-1000 μg/mL; 24-72 h) exhibits dose- and time-dependent cytotoxicity on MOLT-4 and U937 cells[3]. |
| ln Vivo |
Metoprolol (2.5 mg/kg/h; infusion; 11 weeks) decreases atherosclerosis and proinflammatory cytokines in ApoE-/- mice[1]. Metoprolol (15 mg/kg/q12h; i.e., 5 days) exhibits anti-viral and anti-inflammatory properties in a murine model of viral myocarditis caused by the coxsackievirus B3[2]. Metoprolol (2.5 mg/kg; intravenously; three bolus injections) inhibits myocardial apoptosis and significantly reduces the expression of activated caspase-9 protein in coronary microembolization (CME) rats[4]. |
| Cell Assay |
Cell Line: U937 and MOLT-4 cells Concentration: 1, 10, 50, 100, 500 and 1000 μg/mL Incubation Time: 24, 48 and 72 h Result: Significantly reduced the viability of MOLT-4 and U937 cells at 1000 μg/mL (3740.14µM) concentration after 48 hours of incubation; similarly, after 72 hours, the viability of MOLT4 cells at ≥100 μg/ml (≥374.01µM) concentrations and U937 cells at ≥500 μg/ml (≥1870.07µM) concentrations was observed. |
| Animal Protocol |
Male ApoE-/- mice 2.5 mg/kg/h Via osmotic minipumps, 11 weeks |
| ADME/Pharmacokinetics |
Absorption When metoprolol is administered orally, it is almost completely absorbed in the gastrointestinal tract. The maximum serum concentration is achieved 20 min after intravenous administration and 1-2 hours after oral administration. The bioavailability of metoprolol is of 100% when administered intravenously and when administered orally it presents about 50% for the tartrate derivative and 40% for the succinate derivative. The absorption of metoprolol in the form of the tartrate derivative is increased by the concomitant administration of food. Route of Elimination Metoprolol is mainly excreted via the kidneys. From the eliminated dose, less than 5% is recovered unchanged. Volume of Distribution The reported volume of distribution of metoprolol is 4.2 L/kg. Due to the characteristics of metoprolol, this molecule is able to cross the blood-brain barrier and even 78% of the administered drug can be found in cerebrospinal fluid. Clearance The reported clearance rate on patients with normal kidney function is 0.8 L/min. In cirrhotic patients, the clearance rate changes to 0.61 L/min. Plasma levels following oral administration of conventional metoprolol tablets, however, approximate 50% of levels following intravenous adminsitration, indicating about 50% first-pass metabolism... Elimination is mainly by biotransformation in the liver. View More
Metoprolol tartrate is rapidly and almost completely absorbed from the GI tract; absorption of a single oral dose of 20-100 mg is complete in 2.5-3 hours. After an oral dose, about 50% of the drug administered as conventional tablets appears to undergo first-pass metabolism in the liver. Bioavailability of orally administered metoprolol tartrate increases with increased doses, indicating a possible saturable disposition process of low capacity such as tissue binding in the liver. Steady-state oral bioavailability of extended-release tablets of metoprolol succinate given once daily at dosages equivalent to 50-400 mg of metoprolol tartrate is about 77% of that of conventional tablets at corresponding dosages given once daily or in divided doses. Food does not appear to affect bioavailability of metoprolol succinate extended-release tablets. Following a single oral dose as conventional tablets, metoprolol appears in the plasma within 10 minutes and peak plasma concentrations are reached in about 90 minutes. When metoprolol tartrate conventional tablets are administered with food rather than on an empty stomach, peak plasma concentrations are higher and the extent of absorption of the drug is increased. Following oral administration of metoprolol succinate as extended-release tablets, peak plasma metoprolol concentrations are aobut 25-50% of those attained after administration of metoprolol tartrate conventional tablets given once daily or in divided doses. Time to peak concentration is longer with extended-release tablets, with peak plasma coentrations being reached in about 7 hours following administration of such tablets. Plasma concentrations attained 1 hour after an oral dose are linearly related to metoprolol tartrate doses ranging from 50-400 mg as conventional tablets.
Metabolism / Metabolites Metoprolol goes through significant first-pass hepatic metabolism which covers around 50% of the administered dose. The metabolism of metoprolol is mainly driven by the activity of CYP2D6 and to a lesser extent due to the activity of CYP3A4. The metabolism of metoprolol is mainly represented by reactions of hydroxylation and O-demethylation. Metoprolol does not inhibit or enhance its own metabolism. Three main metabolites of the drug are formed by oxidative deamination, O-dealkylation with subsequent oxidation, and aliphatic hydroxylation; these metabolites account for 85% of the total urinary excretion of metabolites. The metabolites apparently do not have appreciable pharmacologic activity. The rate of hydroxylation, resulting in alpha-hydroxymetoprolol, is genetically determined and is subject to considerable interindividual variation. Poor hydroxylators of metoprolol have increased areas under the plasma concentration-time curves, prolonged elimination half-lives (about 7.6 hours), higher urinary concentrations of unchanged drug, and negligible urinary concentrations of alpha-hydroxymetoprolol compared with extensive hydroxylators. Beta-adrenergic blockade of exercise-induced tachycardia persists for at least 24 hours after administration of a single 200-mg oral dose of metoprolol tartrate in poor hydroxylators. Controlled studies have shown that debrisoquine oxidation phenotype is a major determinant of the metabolism, pharmacokinetics and some of the pharmacological actions of metoprolol. The poor metabolizer phenotype is associated with increased plasma drug concentrations, a prolongation of elimination half-life and more intense and sustained beta blockade. Phenotypic differences have also been observed in the pharmacokinetics of the enantiomers of metoprolol. In vivo and in vitro studies have identified some of the metabolic pathways which are subject to the defect, that is alpha-hydroxylation and O-demethylation. PMID:2868819 Metropolol is a racemic mixture of R-and S-enantiomers, and is primarily metabolized by CYP2D6. Biological Half-Life The immediate release formulations of metoprolol present a half-life of about 3-7 hours. The plasma half-life ranges from approximately 3 to 7 hours. |
| Toxicity/Toxicokinetics |
Effects During Pregnancy and Lactation ◉ Summary of Use during Lactation Because of the low levels of metoprolol in breastmilk, amounts ingested by the infant are small and would not be expected to cause any adverse effects in breastfed infants. Studies on the use of metoprolol during breastfeeding have found no adverse reactions in breastfed infants. Monitor breastfed infants for symptoms of beta blockade such as bradycardia and listlessness due to hypoglycemia. ◉ Effects in Breastfed Infants A study of mothers taking beta-blockers during nursing found a numerically, but not statistically significant increased number of adverse reactions in those taking any beta-blocker. Although the ages of infants were matched to control infants, the ages of the affected infants were not stated. Of 6 mothers taking metoprolol, none reported adverse effects in her breastfed infant. A prospective study of pregnant patients taking a beta-blocker asked mothers to complete a questionnaire about postpartum breastfeeding and any side effects in their breastfed infants. Two mothers reported taking metoprolol in unreported dosages while breastfeeding. Neither reported any adverse reactions in their breastfed infants. ◉ Effects on Lactation and Breastmilk Relevant published information on the effects of beta-blockade or metoprolol during normal lactation was not found as of the revision date. A study in 6 patients with hyperprolactinemia and galactorrhea found no changes in serum prolactin levels following beta-adrenergic blockade with propranolol. |
| References |
[1]. Metoprolol reduces proinflammatory cytokines and atherosclerosis in ApoE-/- mice. Biomed Res Int. 2014;2014:548783. [2]. Carvedilol has stronger anti-inflammation and anti-virus effects than metoprolol in murine model with coxsackievirus B3-induced viral myocarditis. Gene. 2014 Sep 1;547(2):195-201. [3]. Cytotoxicity of Metoprolol on Leukemic Cells in Vitro. IJBC 2018; 10(4): 124-129. [4]. Effect of metoprolol on myocardial apoptosis and caspase-9 activation after coronary microembolization in rats. Exp Clin Cardiol. 2013 Spring;18(2):161-5. |
| Additional Infomation |
Metoprolol succinate is an alcohol and a member of phenols. Metoprolol Succinate is the succinate salt form of metoprolol, a cardioselective competitive beta-1 adrenergic receptor antagonist with antihypertensive properties and devoid of intrinsic sympathomimetic activity. Metoprolol succinate antagonizes beta 1-adrenergic receptors in the myocardium, thereby reducing the rate and force of myocardial contraction, and consequently a diminished cardiac output. This agent may also reduce the secretion of renin with subsequent reduction in levels of angiotensin II thus decreasing sympathetic activation, including vasoconstriction, aldosterone secretion. A selective adrenergic beta-1 blocking agent that is commonly used to treat ANGINA PECTORIS; HYPERTENSION; and CARDIAC ARRHYTHMIAS. See also: Metoprolol (has active moiety); Hydrochlorothiazide; metoprolol succinate (component of). |
Solubility Data
| Solubility (In Vitro) |
DMSO: 16.7~100 mg/mL (25.5~153.2 mM) Water: ~100 mg/mL Ethanol: ~5 mg/mL |
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 1.67 mg/mL (2.56 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 16.7 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 1.67 mg/mL (2.56 mM) (saturation unknown) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 16.7 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. Solubility in Formulation 3: ≥ 1.67 mg/mL (2.56 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 16.7 mg/mL clear DMSO stock solution to 900 μL of corn oil and mix evenly. (Please use freshly prepared in vivo formulations for optimal results.) |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 1.5318 mL | 7.6591 mL | 15.3182 mL | |
| 5 mM | 0.3064 mL | 1.5318 mL | 3.0636 mL | |
| 10 mM | 0.1532 mL | 0.7659 mL | 1.5318 mL |