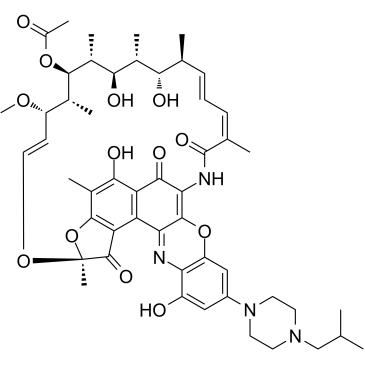
lRifalazil (formerly known as KRM-1648 and AMI-1648) is a rifamycin analog and an antibiotic. Rifalazil kills bacterial cells by blocking off the β-subunit in RNA polymerase. Rifalazil is used as treatments for many different diseases. Of the most common are Chlamydia infection, Clostridium difficile associated diarrhea (CDAD), and tuberculosis (TB).
Physicochemical Properties
| Molecular Formula | C51H64N4O13 |
| Molecular Weight | 941.088 |
| Exact Mass | 940.447 |
| CAS # | 129791-92-0 |
| Related CAS # | 129791-92-0; |
| PubChem CID | 135431094 |
| Appearance | Blue to dark blue solid powder |
| Density | 1.36g/cm3 |
| Boiling Point | 1048.6ºC at 760mmHg |
| Melting Point | 195-200° (dec) |
| Flash Point | 588ºC |
| Vapour Pressure | 0mmHg at 25°C |
| Index of Refraction | 1.634 |
| LogP | 6.573 |
| Hydrogen Bond Donor Count | 5 |
| Hydrogen Bond Acceptor Count | 16 |
| Rotatable Bond Count | 6 |
| Heavy Atom Count | 68 |
| Complexity | 2510 |
| Defined Atom Stereocenter Count | 9 |
| SMILES | C[C@H]1/C=C/C=C(\C(=O)NC2=C3C(=C4C(=C(C(=C5C4=C([C@](O5)(O/C=C/[C@@H]([C@H]([C@H]([C@@H]([C@@H]([C@@H]([C@H]1O)C)O)C)OC(=O)C)C)OC)C)O)C)O)C2=O)N=C6C(=CC(=CC6=O)N7CCN(CC7)CC(C)C)O3)/C |
| InChi Key | UEFHFKKWYKVLDC-HTQYORAHSA-N |
| InChi Code | InChI=1S/C51H64N4O13/c1-24(2)23-54-16-18-55(19-17-54)32-21-33(57)39-35(22-32)67-48-40(52-39)36-37-44(60)30(8)47-38(36)49(62)51(10,68-47)65-20-15-34(64-11)27(5)46(66-31(9)56)29(7)43(59)28(6)42(58)25(3)13-12-14-26(4)50(63)53-41(48)45(37)61/h12-15,20-22,24-25,27-29,34,42-43,46,57-60H,16-19,23H2,1-11H3,(H,53,63)/b13-12+,20-15+,26-14-/t25-,27+,28+,29+,34-,42-,43+,46+,51-/m0/s1 SMILES |
| Chemical Name | (7S,9E,11S,12R,13S,14R,15R,16R,17S,18S,19E,21Z)-2,15,17,32-Tetrahydroxy-30-(4-isobutyl-1-piperazinyl)-11-methoxy-3,7,12,14,16,18,22-heptamethyl-6,23,37-trioxo-8,27,38-trioxa-24,34-diazahexacyclo[23.11.1.14,7.05,36.026,35.028,33]octatriaconta-1(36),2,4,9,19,21,25,28,30,32,34-undecaen-13-yl acetate |
| Synonyms | Rifalazil ABI 1648 ABI1648 ABI -648 Krm-1648 Krm 1648 Krm1648 |
| HS Tariff Code | 2934.99.9001 |
| Storage |
Powder-20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month Note: Please store this product in a sealed and protected environment, avoid exposure to moisture. |
| Shipping Condition | Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs) |
Biological Activity
| Targets |
Bacterial DNA-dependent RNA polymerase (specifically of Chlamydia trachomatis and Chlamydia pneumoniae)[1] |
| ln Vitro |
Rifalazil inhibits Clostridium difficile, Clostridium perfringens, and Bacteroides fragilis, with MIC50 values of 0.0015, 0.0039, and 0.0313 µg/ml, respectively. It shows antibacterial action against Gram-positive gut bacteria [3]. MIC50 values of 16 and 16 µg/ml, respectively, show that rifalazil inhibits Escherichia coli and Klebsiella pneumoniae, two Gram-negative enteric bacteria [3]. The antibacterial activity of Rifalazil is directed against gram-positive bacteria that are not found in the intestinal tract. Specifically, it inhibits the growth of methicillin-sensitive, methicillin-resistant, methicillin-and quinolone-resistant Staphylococcus aureus, and Staphylococcus epidermidis cocci. The MIC50 values of these bacteria are 0.0078, 0.0078, 0.0078, 0.0078, 0.0002, and 0.0001 µg/ml, respectively [3]. With MIC50 values of 0.004, 0.000125, and 0.00025 µg/ml, respectively, rifalazil exhibits antibacterial activity against Helicobacter pylori, Chlamydia pneumoniae, and Chlamydia trachomatis [3]. Rifalazil exhibits potent antibacterial activity against Chlamydia trachomatis and Chlamydia pneumoniae in cell culture. The MICs range from 0.00025 to 0.0025 µg/ml depending on the strain and methodology.[1] Rifalazil demonstrates a unique "protective effect" (PE) where pretreatment of mammalian cell monolayers with the drug protects them against subsequent Chlamydia infection. This effect is significantly stronger and longer-lasting than that of azithromycin, rifampin, doxycycline, and ofloxacin. For example, pretreatment of McCoy cells with 0.002 µg/ml rifalazil for 24 hours protected against challenge with C. trachomatis serovar D 2 days later. The PE lasted 6 to 12 days depending on the cell line.[1] The PE was observed across five different mammalian cell lines (McCoy, HeLa, Hep-2, BGMK, HL) and against various C. trachomatis and C. pneumoniae isolates.[1] The PE is mediated specifically by inhibition of the chlamydial RNA polymerase, as demonstrated using C. trachomatis mutants with altered RNA polymerases (mutants L2/UW-60, L2/UW-73, L2/UW-153). The protective dose for these mutants increased proportionally to their elevated MICs, confirming the target-specific mechanism.[1] |
| ln Vivo |
There was a significant decrease in the number of spleens in each group of mice in which Mycobacterium tuberculosis was detected when rifalazil (oral gavage; 20, 25, and 150 mg/kg; 6-8 weeks) was combined with isoniazid (INH) for at least 6 weeks. This was in contrast to the reduction in early and late controls. Furthermore, the addition of pyrazinamide (PZA) did not significantly improve RLZ-INH treatment at any point in time [2]. In a murine model of tuberculosis, oral treatment with rifalazil in combination with isoniazid (INH) demonstrated potent sterilizing activity. Treatment with rifalazil (20 mg/kg) plus INH (25 mg/kg) for 6 weeks or longer significantly reduced the number of viable M. tuberculosis organisms in the spleens and lungs of infected mice compared to untreated controls, achieving a "nonculturable" state (no detectable colonies from organ homogenates) in some animals.[2] The minimum treatment duration required to achieve and maintain this nonculturable state (i.e., prevent regrowth after therapy cessation) was determined. Treatment with rifalazil plus INH for 6 or 8 weeks led to a nonculturable state immediately after treatment, but regrowth occurred in a significant number of mice during a post-treatment observation period (4 months for the first experiment). A minimum of 10 weeks of rifalazil-INH treatment was necessary to achieve and maintain a nonculturable state through the observation period.[2] The addition of pyrazinamide (PZA) to the rifalazil-INH regimen was evaluated. PZA (150 mg/kg) combined with rifalazil-INH for short-term treatment (3 weeks) resulted in a significantly greater reduction in bacterial counts in both spleens and lungs compared to rifalazil-INH alone at the 3-week time point. However, for longer treatment durations (6, 8, or 10 weeks), the addition of PZA did not significantly shorten the time required to achieve a nonculturable state, nor did it significantly improve the prevention of regrowth after therapy cessation, although a non-statistically significant trend towards reduced regrowth was noted.[2] |
| Cell Assay |
Antimicrobial Susceptibility Testing (MIC Determination): Chlamydia strains were inoculated onto McCoy cell monolayers in 96-well microtiter plates. The inoculum size was 10,000 to 50,000 inclusion-forming units per well. Within 30 minutes of adding chlamydiae, the monolayer was centrifuged at 1,200 × g for 1 hour at 37°C. The supernatant was removed, and growth medium containing 1 µg/ml cycloheximide and the appropriate concentration of rifalazil (or other drugs) was added. Cells were incubated at 37°C in 4% CO₂ for 48 hours, then fixed with methanol. Chlamydial inclusions were detected by fluorescence using a genus-specific monoclonal antibody.[1] Drug Protection Determination (Protective Effect Assay): Monolayers of various mammalian cells (McCoy, HeLa, Hep-2, BGMK, HL) were grown in 48-well plates. Cells were exposed to twofold dilutions of rifalazil (or other drugs) for periods ranging from 5 minutes to 72 hours (24 hours was standard). Cells were then centrifuged, rinsed three times with phosphate-buffered saline, and placed in fresh, antibacterial-free growth medium containing 1 µg/ml cycloheximide. The monolayers were incubated for up to 12 days in the absence of drugs (with medium changes every 48 hours) before being challenged with C. trachomatis or C. pneumoniae at a multiplicity of infection of 0.5. After infection, cells were incubated for 48 hours, fixed, and inclusions were detected by immunofluorescence. The minimal protective concentration was defined as the lowest drug concentration that prevented the formation of morphologically normal inclusions.[1] |
| Animal Protocol |
Animal/Disease Models: Female CD-1 mice infected with 5.2×107 live mycobacteria [2] Doses: 20, 25 and 150 mg/kg; 6-8 weeks Route of Administration: po (oral gavage) Experimental Results: with isoniazid (INH) combination shows its potential for short-term treatment of Mycobacterium tuberculosis infection. Infection Model: Five- to six-week-old female outbred CD-1 mice were infected intravenously via a caudal vein with approximately 10⁷ viable Mycobacterium tuberculosis (strain Erdman) organisms suspended in 0.2 ml of modified 7H10 broth.[2] Treatment Regimen: Treatment began 1 week post-infection and was administered orally by gavage, 5 days per week, for designated periods (e.g., 3, 4, 5, 6, 8, 10, or 12 weeks). Rifalazil was dissolved in dimethyl sulfoxide (DMSO) and then diluted in distilled water, with a final DMSO concentration of 0.5% at administration. The dose of rifalazil was 20 mg/kg of body weight. Isoniazid (INH, 25 mg/kg) and pyrazinamide (PZA, 150 mg/kg) were dissolved in distilled water. Drugs were administered in a dose volume of 0.2 ml.[2] Assessment of Efficacy: At the end of treatment or after a post-treatment observation period (3 or 4 months without therapy), mice were euthanized. Spleens and right lungs were aseptically removed, homogenized, and plated (0.1 ml aliquots of the entire organ homogenate for treatment groups achieving low counts, or titrated for others) on 7H10 agar plates to determine the number of culturable mycobacteria (CFU). Plates were incubated at 37°C in ambient air for 4 weeks before counting.[2] |
| ADME/Pharmacokinetics |
Metabolism / Metabolites The major metabolites of rifalazil in human are 25-deacetyl-benzoxazinorifamycin and 32-hydroxy-benzoxazinorifamycin. The enzyme responsible for the benzoxazinorifamycin-25-deacetylation is a B-esterase while the enzyme responsible for the benzoxazinorifamycin-32-hydroxylation is CYP3A4. Rifalazil is noted to have a long half-life in animals and humans, although specific half-life values are not provided.[1] Rifalazil can enter mammalian cells and concentrate within them, a property contributing to its prolonged protective effect in cell culture.[1] |
| References |
[1]. Rifalazil pretreatment of mammalian cell cultures prevents subsequent Chlamydia infection.Antimicrob Agents Chemother. 2006 Feb;50(2):439-44. [2]. Evaluation of rifalazil in long-term treatment regimens for tuberculosis in mice.Antimicrob Agents Chemother. 2000 Jun;44(6):1458-62. [3]. Development potential of rifalazil.Expert Opin Investig Drugs. 2003 Feb;12(2):255-71. |
| Additional Infomation |
Rifalazil is a phenoxazine. Rifalazil is a derivative of the antibiotic rifamycin. It is being investigated by ActivBiotics for the treatment of various bacterial infections. Drug Indication Investigated for use/treatment in atherosclerosis, bacterial infection, and peripheral vascular disease. Mechanism of Action The potent antimycobacterial activity of rifalazil is due to inhibition of bacterial RNA polymerase. Pharmacodynamics Rifalazil represents a new generation of ansamycins that contain a unique four-ring structure. Originally rifalazil was developed as a therapeutic agent to replace rifampin as part of a multiple drug regimen in the treatment of tuberculosis. As a result of its superior antimicrobial activity and high intracellular levels, rifalazil has potential to treat indications caused by the intracellular pathogen, Chlamydia trachomatis, which causes non-gonococcal urethritis and cervicitis, often leading to pelvic inflammatory disease. Rifalazil also has potential to treat the related microorganism, Chlamydia pneumoniae, which may be involved in chronic inflammatory processes thought to be partly responsible for atherosclerosis. Due to its favourable antimicrobial spectrum and other positive attributes, rifalazil may also prove valuable in the treatment of gastric ulcer disease, caused by Helicobacter pylori, and antibiotic-associated colitis, the result of toxin production following the growth of Clostridium difficile in the colon. The potential value of rifalazil in the treatment of these indications will be assessed in human clinical trials. Rifalazil is a novel rifamycin derivative (3'-hydroxy-5'-(4-isobutyl-1-piperazinyl)benzoxazino-rifamycin) that inhibits bacterial DNA-dependent RNA polymerase.[1] It shows high potency against mycobacteria, gram-positive bacteria, Helicobacter pylori, C. pneumoniae, and C. trachomatis.[1] The unique "protective effect" (PE) of rifalazil suggests that it may provide prolonged protection against reinfection after treatment, which could be of public health value, especially for sexually transmitted and ocular chlamydial infections where reinfection is common.[1] The PE is proposed to be due to rifalazil's ability to concentrate and persist within mammalian cells for extended periods, allowing it to inhibit the RNA polymerase of chlamydiae that infect the cells days after drug removal.[1] |
Solubility Data
| Solubility (In Vitro) | DMSO : ~8.33 mg/mL (~8.85 mM) |
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 2.2 mg/mL (2.34 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 22.0 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 2.2 mg/mL (2.34 mM) (saturation unknown) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 22.0 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. (Please use freshly prepared in vivo formulations for optimal results.) |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 1.0626 mL | 5.3130 mL | 10.6260 mL | |
| 5 mM | 0.2125 mL | 1.0626 mL | 2.1252 mL | |
| 10 mM | 0.1063 mL | 0.5313 mL | 1.0626 mL |