Physicochemical Properties
| Molecular Formula | C15H21NO5CL2 |
| Molecular Weight | 366.23694 |
| Exact Mass | 365.079 |
| CAS # | 119509-24-9 |
| Related CAS # | 119509-24-9; |
| PubChem CID | 54676868 |
| Appearance | White to off-white solid powder |
| Density | 1.3±0.1 g/cm3 |
| Boiling Point | 532.6±50.0 °C at 760 mmHg |
| Flash Point | 275.9±30.1 °C |
| Vapour Pressure | 0.0±3.2 mmHg at 25°C |
| Index of Refraction | 1.534 |
| LogP | -0.8 |
| Hydrogen Bond Donor Count | 2 |
| Hydrogen Bond Acceptor Count | 5 |
| Rotatable Bond Count | 8 |
| Heavy Atom Count | 23 |
| Complexity | 544 |
| Defined Atom Stereocenter Count | 3 |
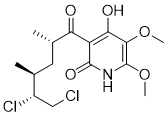
| SMILES | C[C@@H](C[C@H](C)C(=O)C1=C(C(=C(NC1=O)OC)OC)O)[C@H](CCl)Cl |
| InChi Key | OVULNOOPECCZRG-CIUDSAMLSA-N |
| InChi Code | InChI=1S/C15H21Cl2NO5/c1-7(9(17)6-16)5-8(2)11(19)10-12(20)13(22-3)15(23-4)18-14(10)21/h7-9H,5-6H2,1-4H3,(H2,18,20,21)/t7-,8-,9-/m0/s1 |
| Chemical Name | 3-[(2S,4S,5R)-5,6-dichloro-2,4-dimethylhexanoyl]-4-hydroxy-5,6-dimethoxy-1H-pyridin-2-one |
| HS Tariff Code | 2934.99.9001 |
| Storage |
Powder-20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month Note: (1). This product requires protection from light (avoid light exposure) during transportation and storage.(2). Please store this product in a sealed and protected environment (e.g. under nitrogen), avoid exposure to moisture. |
| Shipping Condition | Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs) |
Biological Activity
| Targets |
Mitochondrial Complex II (succinate-ubiquinone oxidoreductase) inhibitor (IC₅₀ ~10 nM) [1] Mitochondrial ATP-sensitive potassium (mK_ATP) channel activator (effective concentration: 1 nM) [1] |
| ln Vitro |
Atpenin A5 has IC50 values of 8.3, 9.3, and 8.5 nM, respectively, for its cytostatic effects on cardiomyocytes, mitochondria, and mitochondrial particles (SMP). Manhattan complex II chip Atpenin A5 (AA5) is a powerful chip. In isolated cardiomyocytes, atpenin A5 (1 nM) mimics reperfusion (IR) injury and inhibits mKATP channel activation [1]. Atpenin A5 (AA5) is a potent and specific inhibitor of mitochondrial complex II. The IC₅₀ values for complex II inhibition were determined to be 8.3 nM in submitochondrial particles (SMPs), 9.3 nM in isolated rat heart mitochondria, and 8.5 nM in isolated rat cardiomyocytes. [1] Atpenin A5 (at 1 nM concentration) activated the mitochondrial ATP-sensitive potassium (mK_ATP) channel in isolated rat heart mitochondria, as measured by a potassium uptake and swelling assay. This activation was sensitive to the mK_ATP channel antagonists 5-hydroxydecanoate (5HD) and glyburide. [1] The dose-response relationship for mK_ATP channel opening by Atpenin A5 showed maximal activation at 1 nM when mitochondria were respiring on complex I-linked substrates (glutamate/malate). When using complex II-linked substrate (succinate), higher concentrations of AA5 (>1 nM) diminished the channel-opening effect, likely due to complex II inhibition limiting membrane potential. [1] In isolated adult rat cardiomyocytes subjected to simulated ischemia-reperfusion (SIR) injury, pretreatment with Atpenin A5 protected cells in a dose-dependent manner, with optimal protection observed at a concentration of 1 nM. This protective effect was blocked by co-treatment with the mK_ATP channel antagonists 5HD (300 µM) or glyburide (2 µM). [1] Atpenin A5 (1 nM) induced mK_ATP channel opening and mitochondrial swelling even in mitochondria respiring on ascorbate plus TMPD (which feeds electrons directly into complex IV), indicating that its effect on the mK_ATP channel is not merely a downstream consequence of complex I or II inhibition. [1] A very high concentration of Atpenin A5 (1 µM) did not inhibit the respiration of mitochondria in the presence of glutamate plus malate (complex I-linked substrates). [1] |
| ln Vivo |
In the postpartum heart following myocardial infarction (MI), inhibition of succinate dehydrogenase by Atpenin A5 promotes cardiomyocyte mitosis and regeneration; in contrast to heart disease, the myocardium in the myocardial infarction area injected with Atpenin A5 becomes thicker and scars are significantly reduced [2]. Atpenin A5 is a valid benchmark for succinate dehydrogenase (SDH). Injection of Atpenin A5 (100 μg/kg daily) starting at postnatal day 7 (P7) in neonatal mice following myocardial infarction (MI) significantly increased the number of cardiomyocytes undergoing mitosis and cytokinesis, as evidenced by increased pH3 and Aurora B staining compared to controls [2]. Treatment with Atpenin A5 also promoted myocardial regeneration, with reduced fibrotic scar size and restoration of cardiac function (ejection fraction, fractional shortening, left ventricular dimensions) at 21 days post-MI [2]. These effects were similar to those observed with malonate, suggesting that SDH inhibition is the central mechanism [2] . |
| Enzyme Assay |
The enzymatic activity of mitochondrial complex II (succinate dehydrogenase) was measured spectrophotometrically. The assay monitored the thenoyltrifluoroacetone-sensitive rate of succinate-driven, coenzyme Q₂-linked reduction of the dye dichlorophenolindophenol (DCPIP). Activity was measured in submitochondrial particles (SMPs), isolated mitochondria, and isolated cardiomyocytes to determine the inhibitory potency (IC₅₀) of Atpenin A5. [1] The activity of the mitochondrial ATP-sensitive potassium (mK_ATP) channel was monitored using a swelling assay. Isolated rat heart mitochondria were suspended in a potassium-based swelling buffer containing oligomycin (to prevent state 3 respiration). Channel activity was assessed by measuring the decrease in light scattering (absorbance at 520 nm) caused by potassium uptake and consequent mitochondrial swelling. The assay validates mK_ATP activity through a specific pharmacological profile: swelling in K⁺ media, inhibition by ATP, reversal of ATP inhibition by mK_ATP agonists (e.g., diazoxide or AA5), and blockade of agonist effects by antagonists (e.g., 5HD or glyburide). No such effects are observed in sodium-based control media. [1] |
| Cell Assay |
Ventricular cardiomyocytes were isolated from adult male Sprague-Dawley rats by perfusion with collagenase. For simulated ischemia-reperfusion (SIR) experiments, approximately 5 x 10⁵ cells were incubated in Krebs-Henseleit buffer with 2% BSA. Cells were subjected to 1 hour of anoxia (95% N₂ / 5% CO₂, glucose-free buffer, pH 6.5) followed by 30 minutes of reoxygenation (95% O₂ / 5% CO₂, glucose-replete buffer, pH 7.4). To test for protection, Atpenin A5 (at concentrations ranging from 0.1 to 100 nM) or other compounds were added to the incubation medium 20 minutes prior to the onset of simulated ischemia. At the end of the reoxygenation period, cell viability was determined by Trypan blue exclusion. [1] |
| Animal Protocol |
Animal/Disease Models: Neonatal mice [2] Doses: 100 μg/kg Route of Administration: Daily injection Experimental Results: Myocardial thickness in the infarct area was Dramatically increased and scar size was diminished compared with the control group. Isolated rat hearts from male Sprague-Dawley rats were perfused in Langendorff (retrograde) mode with Krebs-Henseleit buffer at constant flow. After a 20-minute equilibration period, hearts were subjected to global ischemia (25 minutes) followed by reperfusion (120 minutes). To test the cardioprotective effect, Atpenin A5 was dissolved in DMSO and infused into the perfusion cannula for 20 minutes prior to ischemia, at a final concentration in the perfusate of 50 nM. This was followed by a 30-second washout period before the onset of ischemia. In some groups, the mK_ATP antagonist 5-hydroxydecanoate (5HD, 300 µM) was co-infused with Atpenin A5 starting from the beginning of the protocol. At the end of reperfusion, hearts were sliced, stained with 1% triphenyltetrazolium chloride (TTC) to differentiate infarcted (white) from viable (red) tissue, and infarct size was quantified. Left ventricular function (rate-pressure product) was monitored throughout the protocol via a balloon inserted into the left ventricle. [1] |
| References |
[1]. The complex II inhibitor atpenin A5 protects against cardiac ischemia-reperfusion injury via activation of mitochondrial KATP channels. Basic Res Cardiol. 2009 Mar;104(2):121-9. [2]. Malonate Promotes Adult Cardiomyocyte Proliferation and Heart Regeneration. Circulation. 2021 May 18;143(20):1973-1986. |
| Additional Infomation |
Atpenin A5 has been reported in Streptomyces with data available. Atpenin A5 is identified as the most potent mK_ATP channel opener discovered to date, effective at 1 nM, which is approximately 10,000-fold more potent than the classic opener diazoxide. [1] The cardioprotective mechanism of Atpenin A5 appears to be dependent on mK_ATP channel activation rather than complex II inhibition, because: (1) its optimal protective concentration (1 nM) is an order of magnitude below its IC₅₀ for complex II inhibition (~10 nM), and (2) its protective effects in both cardiomyocytes and isolated hearts are blocked by mK_ATP channel antagonists (5HD and glyburide). [1] The study proposes that complex II protein may play a structural or regulatory role in the mK_ATP channel complex, given the significant pharmacological overlap and the fact that Atpenin A5, a specific complex II inhibitor, is also a potent mK_ATP opener. [1] Administration of Atpenin A5 (50 nM) to isolated perfused hearts caused an immediate but transient decrease in coronary perfusion pressure (vasodilation) and a drop in rate-pressure product, similar to the effects observed with ischemic preconditioning. [1] The literature discussion notes that while Atpenin A5 shows promise as a cardioprotectant in vitro, its potential clinical use may be limited by possible long-term neurodegenerative side effects, as observed with prolonged administration of other mitochondrial complex inhibitors (like malonate or 3-nitropropionic acid) in vivo. The development of cardiac-specific agents may be needed to circumvent such effects. [1] |
Solubility Data
| Solubility (In Vitro) | DMSO : ~100 mg/mL (~273.04 mM) |
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 2.5 mg/mL (6.83 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 2.5 mg/mL (6.83 mM) (saturation unknown) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. Solubility in Formulation 3: ≥ 2.5 mg/mL (6.83 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 900 μL of corn oil and mix evenly. (Please use freshly prepared in vivo formulations for optimal results.) |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 2.7304 mL | 13.6522 mL | 27.3045 mL | |
| 5 mM | 0.5461 mL | 2.7304 mL | 5.4609 mL | |
| 10 mM | 0.2730 mL | 1.3652 mL | 2.7304 mL |