Physicochemical Properties
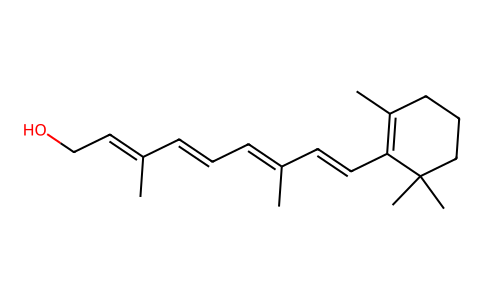
| Molecular Formula | C20H30O |
| Molecular Weight | 286.4516 |
| Exact Mass | 286.229 |
| CAS # | 11103-57-4 |
| PubChem CID | 445354 |
| Appearance | Solvated crystals from polar solvents, such as methanol or ethyl formate |
| Density | 1.0±0.1 g/cm3 |
| Boiling Point | 421.2±14.0 °C at 760 mmHg |
| Melting Point | 62-64ºC |
| Flash Point | 147.3±16.4 °C |
| Vapour Pressure | 0.0±2.3 mmHg at 25°C |
| Index of Refraction | 1.549 |
| LogP | 6.84 |
| Hydrogen Bond Donor Count | 1 |
| Hydrogen Bond Acceptor Count | 1 |
| Rotatable Bond Count | 5 |
| Heavy Atom Count | 21 |
| Complexity | 496 |
| Defined Atom Stereocenter Count | 0 |
| SMILES | OC/C=C(/C=C/C=C(/C=C/C1=C(C)CCCC1(C)C)\C)\C |
| InChi Key | FPIPGXGPPPQFEQ-OVSJKPMPSA-N |
| InChi Code | InChI=1S/C20H30O/c1-16(8-6-9-17(2)13-15-21)11-12-19-18(3)10-7-14-20(19,4)5/h6,8-9,11-13,21H,7,10,14-15H2,1-5H3/b9-6+,12-11+,16-8+,17-13+ |
| Chemical Name | (2E,4E,6E,8E)-3,7-dimethyl-9-(2,6,6-trimethylcyclohexen-1-yl)nona-2,4,6,8-tetraen-1-ol |
| HS Tariff Code | 2934.99.9001 |
| Storage |
Powder-20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month |
| Shipping Condition | Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs) |
Biological Activity
| ADME/Pharmacokinetics |
Absorption, Distribution and Excretion Readily absorbed from the normal gastrointestinal tract Vitamin A is distributed into breast milk ... . Less than 5% of circulating vitamin A is bound to lipoproteins in blood (normal), but may be up to 65% when hepatic stores are saturated because of excessive intake. The amount of vitamin A bound to lipoproteins may be increased in hyperlipoproteinemia. When released from liver, vitamin A is bound to retinol-binding protein (RBP). Most vitamin A circulates in the form of retinol bound to RBP. Storage: Hepatic (approximately 2 years' adult requirements), with small amounts stored in kidney and lung tissues. Zinc is required for mobilization of vitamin A reserves in the liver. More than 90% of the intake of preformed vitamin A is in the form of retinol esters, usually as retinyl palmitate. ... When a large excess is ingested, some of the vitamin escapes in the feces. ... Absorption ... is related to that of lipid and is enhanced by bile. ... Aqueous dispersions ... are absorbed more rapidly than are oily solution. For more Absorption, Distribution and Excretion (Complete) data for VITAMIN A (9 total), please visit the HSDB record page. Metabolism / Metabolites Hepatic. Retinol is conjugated with glucuronic acid; the B-glucuronide undergoes enterohepatic circulation and oxidation to retinol and retinoic acid. Retinoic acid undergoes decarboxylation and conjugation with glucuronic acid. Retinol is converted to retinyl phosphate in epithelial tissues, and this intermediate is in turn metabolized to mannosylretinylphosphate in a reaction that is catalyzed by a microsomal enzyme and requires guanosine diphosphomannose as a glycosyl donor. ... /the vitamin A/ mediates transfer of mannose to specific glycoproteins. Retinol is in part conjugated to form a beta-glucuronide, which undergoes enterohepatic circulation and is oxidized to retinal and retinoic acid. Within the retina, all-trans-retinol is oxidized to retinal by alcohol dehydrogenases, and is then Isomerized to the 11-cis-isomer which combines with opsin in the rod to yield rhodopsin, and with different opsins in human cones to yield three different iodopsin pigments. Retinoic acid (RA) is the bioactive metabolite of vitamin A (retinol) which acts on cells to establish or change the pattern of gene activity. Retinol is converted to RA by the action of two types of enzyme, retinol dehydrogenases and retinal dehydrogenases. In the nucleus RA acts as a ligand to activate two families of transcription factors, the RA receptors (RAR) and the retinoid X receptors (RXR) which heterodimerize and bind to the upstream sequences of RA-responsive genes. Retinol has known human metabolites that include retinal and 4-Hydroxyretinol. Hepatic. Retinol is conjugated with glucuronic acid; the B-glucuronide undergoes enterohepatic circulation and oxidation to retinol and retinoic acid. Retinoic acid undergoes decarboxylation and conjugation with glucuronic acid. Half Life: 1.9 hours Biological Half-Life 1.9 hours Hepatic reserves of vitamin A decrease with a half-life of about 50 days in animals ... |
| Toxicity/Toxicokinetics |
Toxicity Summary Vision:Vitamin A (all-trans retinol) is converted in the retina to the 11-cis-isomer of retinaldehyde or 11-cis-retinal. 11-cis-retinal functions in the retina in the transduction of light into the neural signals necessary for vision. 11-cis-retinal, while attached to opsin in rhodopsin is isomerized to all-trans-retinal by light. This is the event that triggers the nerve impulse to the brain which allows for the perception of light. All-trans-retinal is then released from opsin and reduced to all-trans-retinol. All-trans-retinol is isomerized to 11-cis-retinol in the dark, and then oxidized to 11-cis-retinal. 11-cis-retinal recombines with opsin to re-form rhodopsin. Night blindness or defective vision at low illumination results from a failure to re-synthesize 11-cis retinal rapidly. Epithelial differentiation: The role of Vitamin A in epithelial differentiation, as well as in other physiological processes, involves the binding of Vitamin A to two families of nuclear retinoid receptors (retinoic acid receptors, RARs; and retinoid-X receptors, RXRs). These receptors function as ligand-activated transcription factors that modulate gene transcription. When there is not enough Vitamin A to bind these receptors, natural cell differentiation and growth are interrupted. Interactions Insulin antagonizes the /teratogenic/ effects /of vitamin A/. The antithyroid compound methylthiouracil increases teratogenic effect /of vitamin A/. Thyroxine antagonizes the teratogenic action of vitamin A. In rats, the incidence of congenital abnormalities in the head due to hypervitaminosis A was increased greatly by appropriate administration of cortisone to the dams. For more Interactions (Complete) data for VITAMIN A (19 total), please visit the HSDB record page. Non-Human Toxicity Values LD50 Mouse ip 1510 mg/kg (10 day) LD50 Mouse oral 2570 mg/kg (10 day) LD50 Hen oral 3.15 - 3.7 g/kg body weight |
| Additional Infomation |
Therapeutic Uses Vitamin A is indicated only for prevention or treatment of vitamin A deficiency states. Vitamin A deficiency may occur as a result of inadequate nutrition or intestinal malabsorption but does not occur in healthy individual receiving an adequate balanced diet. For prophylaxis of vitamin A deficiency, dietary improvement, rather than supplementation, is advisable. For treatment of vitamin A deficiency, supplementation is preferred. /Included in US product labeling/ Recommended intakes may be increased and/or supplementation may be necessary in infants receiving unfortified formula or in individuals with the following conditions (based on documented vitamin A deficiency): Diarrhea; gastrectomy; hyperthyroidism; infections, chronic; intestinal diseases: celiac, diarrhea, topical sprue, regional enteritis; malabsorption syndromes associated with pancreatic insufficiency: pancreatic disease, cystic fibrosis; measles; protein deficiency, severe, stress, prolonged; xerophthalmia. /Included in US product labeling/ Some unusual diets (e.g., reducing diets that drastically restrict food selection, especially the fat-containing foods) may not supply minimum daily recommended intakes of vitamin A. Supplementation is necessary in patients receiving total parenteral nutrition (TPN) or undergoing rapid weight loss or in those with malnutrition, because of inadequate dietary intake. Recommended intakes for most vitamins and minerals are increased during pregnancy. Many physicians recommend that pregnant women receive multivitamin and mineral supplements, especially those pregnant women who do not consume an adequate diet and those in high-risk categories (i.e., women carrying more than one fetus, heavy cigarette smokers, and alcohol and drug abusers). Taking excessive amounts of a multivitamin and mineral supplement may be harmful to the mother and/or fetus and should be avoided. For more Therapeutic Uses (Complete) data for VITAMIN A (7 total), please visit the HSDB record page. Drug Warnings Pregnancy risk category: X /CONTRAINDICATED IN PREGNANCY. Studies in animals or humans, or investigational or post-marketing reports, have demonstrated positive evidence of fetal abnormalities or risk which clearly outweights any possible benefit to the patient./ /Parenteral vitamin A/ Doses of vitamin A that do not exceed the physiologic requirement are usually nontoxic. There are insufficient data to show that vitamin A may reduce the occurrence of certain types of cancer. ... Vitamin A has not been proven effective for treatment of renal calculi, hyperthyroidism, anemia, degenerative conditions of the nervous system, sunburn, lung diseases, deafness, osteoarthritis, inflammatory bowel disease, or psoriasis. For more Drug Warnings (Complete) data for VITAMIN A (9 total), please visit the HSDB record page. Pharmacodynamics Vitamin A is effective for the treatment of Vitamin A deficiency. Vitamin A refers to a group of fat-soluble substances that are structurally related to and possess the biological activity of the parent substance of the group called all-trans retinol or retinol. Vitamin A plays vital roles in vision, epithelial differentiation, growth, reproduction, pattern formation during embryogenesis, bone development, hematopoiesis and brain development. It is also important for the maintenance of the proper functioning of the immune system. |
Solubility Data
| Solubility (In Vitro) | May dissolve in DMSO (in most cases), if not, try other solvents such as H2O, Ethanol, or DMF with a minute amount of products to avoid loss of samples |
| Solubility (In Vivo) |
Note: Listed below are some common formulations that may be used to formulate products with low water solubility (e.g. < 1 mg/mL), you may test these formulations using a minute amount of products to avoid loss of samples. Injection Formulations (e.g. IP/IV/IM/SC) Injection Formulation 1: DMSO : Tween 80: Saline = 10 : 5 : 85 (i.e. 100 μL DMSO stock solution → 50 μL Tween 80 → 850 μL Saline) *Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH ₂ O to obtain a clear solution. Injection Formulation 2: DMSO : PEG300 :Tween 80 : Saline = 10 : 40 : 5 : 45 (i.e. 100 μL DMSO → 400 μLPEG300 → 50 μL Tween 80 → 450 μL Saline) Injection Formulation 3: DMSO : Corn oil = 10 : 90 (i.e. 100 μL DMSO → 900 μL Corn oil) Example: Take the Injection Formulation 3 (DMSO : Corn oil = 10 : 90) as an example, if 1 mL of 2.5 mg/mL working solution is to be prepared, you can take 100 μL 25 mg/mL DMSO stock solution and add to 900 μL corn oil, mix well to obtain a clear or suspension solution (2.5 mg/mL, ready for use in animals). Injection Formulation 4: DMSO : 20% SBE-β-CD in saline = 10 : 90 [i.e. 100 μL DMSO → 900 μL (20% SBE-β-CD in saline)] *Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. Injection Formulation 5: 2-Hydroxypropyl-β-cyclodextrin : Saline = 50 : 50 (i.e. 500 μL 2-Hydroxypropyl-β-cyclodextrin → 500 μL Saline) Injection Formulation 6: DMSO : PEG300 : castor oil : Saline = 5 : 10 : 20 : 65 (i.e. 50 μL DMSO → 100 μLPEG300 → 200 μL castor oil → 650 μL Saline) Injection Formulation 7: Ethanol : Cremophor : Saline = 10: 10 : 80 (i.e. 100 μL Ethanol → 100 μL Cremophor → 800 μL Saline) Injection Formulation 8: Dissolve in Cremophor/Ethanol (50 : 50), then diluted by Saline Injection Formulation 9: EtOH : Corn oil = 10 : 90 (i.e. 100 μL EtOH → 900 μL Corn oil) Injection Formulation 10: EtOH : PEG300:Tween 80 : Saline = 10 : 40 : 5 : 45 (i.e. 100 μL EtOH → 400 μLPEG300 → 50 μL Tween 80 → 450 μL Saline) Oral Formulations Oral Formulation 1: Suspend in 0.5% CMC Na (carboxymethylcellulose sodium) Oral Formulation 2: Suspend in 0.5% Carboxymethyl cellulose Example: Take the Oral Formulation 1 (Suspend in 0.5% CMC Na) as an example, if 100 mL of 2.5 mg/mL working solution is to be prepared, you can first prepare 0.5% CMC Na solution by measuring 0.5 g CMC Na and dissolve it in 100 mL ddH2O to obtain a clear solution; then add 250 mg of the product to 100 mL 0.5% CMC Na solution, to make the suspension solution (2.5 mg/mL, ready for use in animals). Oral Formulation 3: Dissolved in PEG400 Oral Formulation 4: Suspend in 0.2% Carboxymethyl cellulose Oral Formulation 5: Dissolve in 0.25% Tween 80 and 0.5% Carboxymethyl cellulose Oral Formulation 6: Mixing with food powders Note: Please be aware that the above formulations are for reference only. InvivoChem strongly recommends customers to read literature methods/protocols carefully before determining which formulation you should use for in vivo studies, as different compounds have different solubility properties and have to be formulated differently. (Please use freshly prepared in vivo formulations for optimal results.) |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 3.4910 mL | 17.4551 mL | 34.9101 mL | |
| 5 mM | 0.6982 mL | 3.4910 mL | 6.9820 mL | |
| 10 mM | 0.3491 mL | 1.7455 mL | 3.4910 mL |