Physicochemical Properties
| Molecular Formula | C43H74N2O14 |
| Molecular Weight | 843.052660000001 |
| Exact Mass | 842.514 |
| CAS # | 24916-50-5 |
| PubChem CID | 5289394 |
| Appearance | Off-white to light yellow solid powder |
| Density | 1.21g/cm3 |
| Boiling Point | 913.7ºC at 760mmHg |
| Melting Point | 134-137ºC |
| Flash Point | 506.4ºC |
| LogP | 2.325 |
| Hydrogen Bond Donor Count | 4 |
| Hydrogen Bond Acceptor Count | 16 |
| Rotatable Bond Count | 11 |
| Heavy Atom Count | 59 |
| Complexity | 1370 |
| Defined Atom Stereocenter Count | 19 |
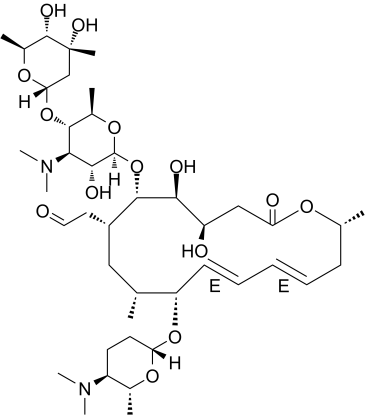
| SMILES | C[C@@H]1C/C=C/C=C/[C@@H]([C@@H](C[C@@H]([C@@H]([C@H]([C@@H](CC(=O)O1)O)OC)O[C@H]2[C@@H]([C@H]([C@@H]([C@H](O2)C)O[C@H]3C[C@@]([C@H]([C@@H](O3)C)O)(C)O)N(C)C)O)CC=O)C)O[C@H]4CC[C@@H]([C@H](O4)C)N(C)C |
| InChi Key | ACTOXUHEUCPTEW-CEUOBAOPSA-N |
| InChi Code | InChI=1S/C43H74N2O14/c1-24-21-29(19-20-46)39(59-42-37(49)36(45(9)10)38(27(4)56-42)58-35-23-43(6,51)41(50)28(5)55-35)40(52-11)31(47)22-33(48)53-25(2)15-13-12-14-16-32(24)57-34-18-17-30(44(7)8)26(3)54-34/h12-14,16,20,24-32,34-42,47,49-51H,15,17-19,21-23H2,1-11H3/b13-12+,16-14+/t24-,25-,26-,27-,28+,29+,30+,31-,32+,34+,35+,36-,37-,38-,39+,40+,41+,42+,43-/m1/s1 |
| Chemical Name | 2-[(4R,5S,6S,7R,9R,10R,11E,13E,16R)-6-[(2S,3R,4R,5S,6R)-5-[(2S,4R,5S,6S)-4,5-dihydroxy-4,6-dimethyloxan-2-yl]oxy-4-(dimethylamino)-3-hydroxy-6-methyloxan-2-yl]oxy-10-[(2R,5S,6R)-5-(dimethylamino)-6-methyloxan-2-yl]oxy-4-hydroxy-5-methoxy-9,16-dimethyl-2-oxo-1-oxacyclohexadeca-11,13-dien-7-yl]acetaldehyde |
| HS Tariff Code | 2934.99.9001 |
| Storage |
Powder-20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month |
| Shipping Condition | Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs) |
Biological Activity
| ADME/Pharmacokinetics |
Absorption, Distribution and Excretion The extent of absorption of Spiramycin was shown to be incomplete. Oral bioavailability ranges from 30-39%. Spiramycin has slower rate of absorption than Erythromycin. It has a high pKa (7.9) which could be a result of high degree of ionization in acidic medium of the stomach. Fecal-biliary route is the primary route of elimination. The secondary route is renal-urinary route. The tissue distribution of spiramycin is extensive. The volume of distribution is in excess of 300 L, and concentrations achieved in bone, muscle, respiratory tract and saliva exceed those found in serum. Spiramycin showed high concentrations in tissues such as: lungs, bronchi, tonsils, and sinuses. 80% of the administered dose excreted in the bile, which makes the fecal-biliary route is the most important route of elimination. Enterohepatic recycling could also occur. Only 4 to 14% of an administered dose is eliminated through renal-urinary excretion route. Spiramycin is well absorbed in humans after oral administration. Oral administration of 15-30 mg/kg bw to healthy young male adults resulted in peak plasma levels in 3-4 hours and plasma concentrations of 0.96-1.65 mg/l. After intravenous dosing (7.25 mg/kg b.w.) a large volume of distribution (Vdss 5.6 l/kg) was observed indicating extensive tissue distribution. Biotransformation did not appear to be important. Biliary excretion was the main route of excretion; only 7-20% of an oral dose was excreted in the urine. Spiramycin is known to achieve high tissue:serum concentrations in pulmonary and prostatic tissues, and in skin. Spiramycin crosses the placenta to the fetus. Concns of the antibiotic in maternal serum, cord blood, & the placenta after a dosage regimen of 2 g/day were 1.19 ug/ml, 0.63 ug/ml, & 2.75 ug/ml, respectively. When the maternal dose was increased to 3 g/day, the levels were 1.69 ug/ml, 0.78 ug/ml, & 6.2 ug/ml, respectively. Based on these results, the cord:maternal serum ratio is approx 0.5. Moreover, at these doses, spiramycin is concentrated in the placenta with levels approx 2-4 times those in the maternal serum. ... Spiramycin is excreted into breast milk. Nursing infants of mothers receiving 1.5 g/day for 3 days had spiramycin serum concns of 20 ug/ml. This concn was bacteriostatic. /MILK/ Spiramycin is a macrolide antibiotic that is active against most of the microorganisms isolated from the milk of mastitic cows. This work investigated the disposition of spiramycin in plasma & milk after iv, intramuscular & subcutaneous admin. Twelve healthy cows were given a single injection of spiramycin at a dose of 30,000 IU/kg by each route. Plasma & milk were collected post injection. Spiramycin concn in the plasma was determined by a high performance liquid chromatography method, & in the milk by a microbiological method. The mean residence time after iv admin was significantly longer (P<0.01) in the milk (20.7 +/- 2.7 h) than in plasma (4.0 +/- 1.6 h). An average milk-to-plasma ratio of 36.5 +/- 15 was calculated from the area concn-time curves. Several pharmacokinetic parameters were examined to determine the bioequivalence of the two extravascular routes. The dose fraction adsorbed after intramuscular or subcutaneous admin was almost 100% & was bioequivalent for the extravascular routes, but the rates of absorption, the max concns & the time to obtain them differed significantly between the two routes. Spiramycin quantities excreted in milk did not differ between the two extravascular routes but the latter were not bioequivalent for max concn in the milk. However, the two routes were bio-equivalent for the duration of time the milk concn exceeded the minimal inhibitory concn (MIC) of various pathogens causing infections in the mammary gland. Plasma protein binding ranges from 10 to 25%. An oral dose of 6 million units produces peak blood concentrations of 3.3 ug/mL after 1.5 to 3 hours; the half life is about 5 to 8 hours. High tissue concentrations are achieved and persist long after the plasma concentration has fallen to low levels. For more Absorption, Distribution and Excretion (Complete) data for SPIRAMYCIN (13 total), please visit the HSDB record page. Metabolism / Metabolites Spiramycin is less metabolised than some of the other macrolides. Metabolism has not been well studied. It is mainly done in the liver to the active metabolites. In cattle, the metabolite neospiramycin, the demycarosyl derivative, is formed. Concentrations of neospiramycin in muscle and kidney were marginally higher than those of spiramycin 14-28 days after dosing; in muscle, levels of neospiramycin and spiramycin were approximately equal. Spiramycin is metabolized in the liver to active metabolites; substantial amounts are excreted in the bile and about 10% in the urine. Biological Half-Life Intravenous: Young persons (18 to 32 years of age): Approximately 4.5 to 6.2 hours. Elderly persons (73 to 85 years of age): Approximately 9.8 to 13.5 hours. Oral: 5.5-8 hours, Rectal in children: 8 hours An oral dose of 6 million units produces ... /a/ half life is about 5 to 8 hours. |
| Toxicity/Toxicokinetics |
Protein Binding Low level of protein binding (10-25%). |
| References |
[1]. Hydroxylation and hydrolysis: two main metabolic ways of spiramycin I in anaerobic digestion. Bioresour Technol. 2014 Feb;153:95-100. |
| Additional Infomation |
Spiramycin is a primarily bacteriostatic macrolide antimicrobial agent with activity against Gram-positive cocci and rods, Gram-negative cocci and also Legionellae, mycoplasmas, chlamydiae, some types of spirochetes, Toxoplasma gondii and Cryptosporidium. Spiramycin is a 16-membered ring macrolide discovered in 1952 as a product of Streptomyces ambofaciens that has been available in oral formulations since 1955, and parenteral formulations since 1987. Resistant organisms include Enterobacteria, pseudomonads, and moulds. Spiramycin is a macrolide originally discovered as product of Streptomyces ambofaciens, with antibacterial and antiparasitic activities. Although the specific mechanism of action has not been characterized, spiramycin likely inhibits protein synthesis by binding to the 50S subunit of the bacterial ribosome. This agent also prevents placental transmission of toxoplasmosis presumably through a different mechanism, which has not yet been characterized. Drug Indication Macrolide antibiotic for treatment of various infections. Mechanism of Action The mechanism of action of macrolides has been a matter of controversy for some time. Spiramycin, a 16-membered macrolide, inhibits translocation by binding to bacterial 50S ribosomal subunits with an apparent 1 : 1 stoichiometry. This antibiotic is a potent inhibitor of the binding to the ribosome of both donor and acceptor substrates. The primary mechanism of action is done by stimulation of dissociation of peptidyl-tRNA from ribosomes during translocation.I |
Solubility Data
| Solubility (In Vitro) | DMSO : ~100 mg/mL (~118.62 mM) |
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 2.5 mg/mL (2.97 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 2.5 mg/mL (2.97 mM) (saturation unknown) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. Solubility in Formulation 3: ≥ 2.5 mg/mL (2.97 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 900 μL of corn oil and mix evenly. (Please use freshly prepared in vivo formulations for optimal results.) |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 1.1862 mL | 5.9308 mL | 11.8617 mL | |
| 5 mM | 0.2372 mL | 1.1862 mL | 2.3723 mL | |
| 10 mM | 0.1186 mL | 0.5931 mL | 1.1862 mL |