Physicochemical Properties
| Molecular Formula | C8H18N4O2 |
| Molecular Weight | 202.25412 |
| Exact Mass | 202.143 |
| CAS # | 30344-00-4 |
| PubChem CID | 169148 |
| Appearance | White to off-white solid powder |
| Density | 1.22g/cm3 |
| Boiling Point | 367.7ºC at 760mmHg |
| Flash Point | 176.2ºC |
| Index of Refraction | 1.54 |
| LogP | 0.455 |
| Hydrogen Bond Donor Count | 4 |
| Hydrogen Bond Acceptor Count | 4 |
| Rotatable Bond Count | 7 |
| Heavy Atom Count | 14 |
| Complexity | 206 |
| Defined Atom Stereocenter Count | 1 |
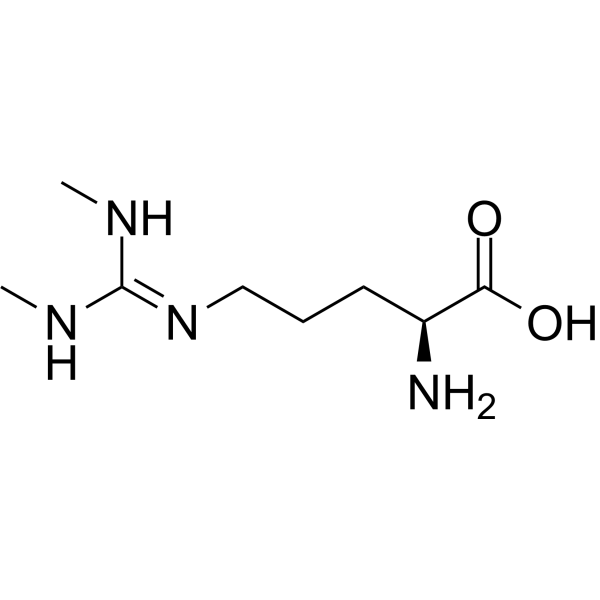
| SMILES | N[C@@H](CCCN/C(NC)=N/C)C(O)=O |
| InChi Key | HVPFXCBJHIIJGS-LURJTMIESA-N |
| InChi Code | InChI=1S/C8H18N4O2/c1-10-8(11-2)12-5-3-4-6(9)7(13)14/h6H,3-5,9H2,1-2H3,(H,13,14)(H2,10,11,12)/t6-/m0/s1 |
| Chemical Name | (2S)-2-amino-5-[(N,N'-dimethylcarbamimidoyl)amino]pentanoic acid |
| HS Tariff Code | 2934.99.9001 |
| Storage |
Powder-20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month |
| Shipping Condition | Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs) |
Biological Activity
| Targets |
SDMA targets nitric oxide synthase (NOS) (competitive inhibitor)[2][4] |
| ln Vitro |
As an endogenous index of renal function, SDMA is a structural isomer of asymmetric dimethylarginine, a cardiovascular risk factor. SDMA is a rival for arginine transport but does not directly block NOS. A promising endogenous measure of glomerular filtration rate, SDMA is mostly excreted by the kidneys [1]. While SDMA has no effect on the protein expression of NOS, it dose-dependently suppresses the production of NO in intact endothelial cells [1]. Through the activation of NF-κB and subsequent upregulation of IL-6 and TNF-α production, SDMA contributes to the inflammatory process associated with chronic kidney disease [2]. SDMA acts as a proinflammatory agent in vitro, inducing the secretion of proinflammatory cytokines (IL-6, TNF-α) and chemokines (MCP-1) in human umbilical vein endothelial cells (HUVECs) and peripheral blood mononuclear cells (PBMCs) isolated from chronic kidney disease (CKD) patients; treatment with 10-100 μM SDMA for 24 hours increases IL-6 secretion by 2.1-3.5 fold and TNF-α by 1.8-2.9 fold[2] SDMA inhibits NOS activity in endothelial cells, reducing nitric oxide (NO) production by 30-45% at 50 μM concentration[2][4] |
| ln Vivo |
Both serum and plasma samples of SDMA exhibit good stability, and the assay performs exceptionally well analytically. While SDMA stays constant in dogs who are not affected, it increases in dogs that are afflicted as the disease progresses and is closely correlated with increases in sCr and decreases in GFR [3]. After four weeks, mice receiving a chronic SDMA infusion showed a substantial rise in SDMA levels but no change in GFR. There were no histological alterations seen, particularly in terms of fibrosis or the expression of nitric oxide synthase in endothelial cells. Systolic blood pressure and ejection fraction are unaffected by SDMA [4]. SDMA is a sensitive marker for early detection of chronic kidney disease (CKD) in dogs; serum SDMA levels are significantly elevated in dogs with incipient CKD (glomerular filtration rate [GFR] 30-60 mL/min/1.73m²) compared to healthy dogs, with an area under the ROC curve (AUC) of 0.92[3] Chronic infusion of SDMA in C57BL6/J mice (10 mg/kg/day via osmotic minipump for 4 weeks) reduces GFR by 28%, increases systolic blood pressure by 15-20 mmHg, and induces mild renal interstitial fibrosis without significant changes in myocardial function[4] In humans, serum SDMA levels correlate positively with the extent of coronary artery disease (CAD) and negatively with renal function; patients with multi-vessel CAD have 2.3-fold higher SDMA levels than those with single-vessel CAD[1] In CKD patients, elevated serum SDMA levels are associated with increased systemic inflammation, as indicated by positive correlations with IL-6, TNF-α, and C-reactive protein (CRP) levels[2] |
| Enzyme Assay |
For NOS activity inhibition assay: Culture HUVECs in EBM-2 medium; treat cells with SDMA (10-100 μM) for 24 hours; lyse cells and prepare cytosolic extracts; mix extracts with L-arginine (substrate), NADPH, and cofactors in assay buffer; incubate at 37°C for 60 minutes; measure NO production via Griess reagent or NO-sensitive electrode to assess NOS activity inhibition[2] For cytokine secretion assay: Isolate PBMCs from CKD patients via density gradient centrifugation; culture PBMCs in RPMI 1640 medium; treat with SDMA (10-100 μM) for 24-48 hours; collect culture supernatants; quantify IL-6, TNF-α, and MCP-1 levels via ELISA[2] |
| Cell Assay |
For endothelial cell inflammation assay: Culture HUVECs in EBM-2 medium supplemented with growth factors; seed cells in 6-well plates; treat with SDMA (10-100 μM) for 24 hours; extract total RNA and perform PCR to detect IL-6, TNF-α, and MCP-1 mRNA expression; measure protein levels in cell lysates and supernatants via Western blot and ELISA, respectively[2] |
| Animal Protocol |
For mouse chronic infusion assay: Use male C57BL6/J mice (8-10 weeks old); implant osmotic minipumps subcutaneously to deliver SDMA at 10 mg/kg/day or vehicle (saline) for 4 weeks; measure GFR via inulin clearance before and after treatment; monitor systolic blood pressure weekly using a tail-cuff system; after sacrifice, collect kidneys for histopathological analysis (Masson's trichrome staining for fibrosis) and hearts for echocardiographic assessment[4] For canine CKD marker evaluation assay: Recruit healthy dogs (n=30) and dogs with CKD (n=50, stratified by GFR); collect fasting serum samples; store samples at -80°C until analysis; measure serum SDMA levels via validated immunoassay; correlate SDMA levels with GFR (measured via iohexol clearance) and other renal biomarkers[3] |
| ADME/Pharmacokinetics |
Metabolism / Metabolites Uremic toxins tend to accumulate in the blood either through dietary excess or through poor filtration by the kidneys. Most uremic toxins are metabolic waste products and are normally excreted in the urine or feces. SDMA is an endogenous metabolite of arginine, formed by protein arginine methyltransferases (PRMTs) and released during protein degradation[2][4] SDMA is primarily excreted via the kidneys; renal clearance of SDMA is proportional to GFR, with minimal tubular secretion or reabsorption[3][4] In healthy dogs, the elimination half-life of SDMA is approximately 2.8 hours; in CKD dogs, half-life is prolonged to 4.5-6.2 hours depending on GFR reduction[3] |
| Toxicity/Toxicokinetics |
Toxicity Summary Uremic toxins such as symmetric dimethylarginine are actively transported into the kidneys via organic ion transporters (especially OAT3). Increased levels of uremic toxins can stimulate the production of reactive oxygen species. This seems to be mediated by the direct binding or inhibition by uremic toxins of the enzyme NADPH oxidase (especially NOX4 which is abundant in the kidneys and heart) (A7868). Reactive oxygen species can induce several different DNA methyltransferases (DNMTs) which are involved in the silencing of a protein known as KLOTHO. KLOTHO has been identified as having important roles in anti-aging, mineral metabolism, and vitamin D metabolism. A number of studies have indicated that KLOTHO mRNA and protein levels are reduced during acute or chronic kidney diseases in response to high local levels of reactive oxygen species (A7869). SDMA induces renal interstitial fibrosis in mice after chronic infusion (4 weeks), characterized by increased collagen deposition and α-smooth muscle actin (α-SMA) expression in renal interstitium[4] Elevated SDMA levels contribute to endothelial dysfunction and hypertension via NOS inhibition and reduced NO bioavailability[4] In CKD patients, chronic SDMA elevation is associated with increased cardiovascular risk (CAD, hypertension) and systemic inflammation[1][2] |
| References |
[1]. Symmetrical dimethylarginine: a new combined parameter for renal function and extent ofcoronary artery disease. [2]. Symmetric dimethylarginine as a proinflammatory agent in chronic kidney disease.Clin J Am Soc Nephrol. 2011 Oct;6(10):2374-83. [3]. Symmetric Dimethylarginine Assay Validation, Stability, and Evaluation as a Marker for the EarlyDetection of Chronic Kidney Disease in Dogs. J Vet Intern Med. 2015 Jul-Aug;29(4):1036-44. [4]. Effects of chronic SDMA infusion on glomerular filtration rate, blood pressure, myocardial function and renal histology in C57BL6/J mice. Nephrol Dial Transplant. 2013 Jun;28(6):1434-9. |
| Additional Infomation |
N(omega),N'(omega)-dimethyl-L-arginine is a L-arginine derivative having two methyl groups at the N(omega)- and N'(omega)-positions It has a role as an EC 1.14.13.39 (nitric oxide synthase) inhibitor. It is a member of guanidines, a non-proteinogenic L-alpha-amino acid, a L-arginine derivative and a dimethylarginine. It is a conjugate base of a N(omega),N('omega)-dimethyl-L-argininium(1+). It is a tautomer of a N(omega),N'(omega)-dimethyl-L-arginine zwitterion. Symmetric Dimethylarginine is a dimethylated derivative of L-arginine where the two methyl groups are attached to arginine in a symmetrical configuration. Symmetric dimethylarginine (SDMA) is formed when S-adenosylmethionine protein N-methyltransferases transfer one methyl group from S-adenosylmethionine to each of the two guanidine nitrogen groups of a single arginine residue in a protein. SDMA is released when the protein is degraded. SDMA doesn't bind nitric oxide synthase (NOS) but may noncompetitivelty inhibit nitric oxide (NO) synthesis by reducing L-arginine availability; it also may play a role in the modulation of cardiovascular homeostasis and renal function. Symmetric dimethylarginine is a uremic toxin. Uremic toxins can be subdivided into three major groups based upon their chemical and physical characteristics: 1) small, water-soluble, non-protein-bound compounds, such as urea; 2) small, lipid-soluble and/or protein-bound compounds, such as the phenols and 3) larger so-called middle-molecules, such as beta2-microglobulin. Chronic exposure of uremic toxins can lead to a number of conditions including renal damage, chronic kidney disease and cardiovascular disease. Symmetric dimethylarginine (SDMA) is an endogenously produced inhibitor of nitric oxide synthase (EC-Number 1.14.13.39). However, elevated levels of SDMA occur in patients with vascular disease, especially suffering end-stage renal disease. (A3290). SDMA is a symmetrically dimethylated derivative of L-arginine, structurally similar to asymmetric dimethylarginine (ADMA), but with higher specificity as a renal function marker[3][4] Unlike ADMA, SDMA does not undergo metabolism by dimethylarginine dimethylaminohydrolase (DDAH); its plasma levels are solely regulated by renal excretion[3][4] SDMA serves as a combined parameter for renal function and CAD extent in humans, with higher diagnostic value for early CKD than serum creatinine in dogs[1][3] The proinflammatory mechanism of SDMA involves activation of NF-κB signaling pathway in endothelial cells and immune cells[2] |
Solubility Data
| Solubility (In Vitro) |
DMSO : ~67.5 mg/mL (~333.75 mM) H2O : ~50 mg/mL (~247.22 mM) |
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 2.5 mg/mL (12.36 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 2.5 mg/mL (12.36 mM) (saturation unknown) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 3: 2.5 mg/mL (12.36 mM) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), suspension solution; with ultrasonication. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 900 μL of corn oil and mix evenly. Solubility in Formulation 4: 120 mg/mL (593.33 mM) in PBS (add these co-solvents sequentially from left to right, and one by one), clear solution; with ultrasonication. (Please use freshly prepared in vivo formulations for optimal results.) |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 4.9444 mL | 24.7219 mL | 49.4438 mL | |
| 5 mM | 0.9889 mL | 4.9444 mL | 9.8888 mL | |
| 10 mM | 0.4944 mL | 2.4722 mL | 4.9444 mL |