Physicochemical Properties
| Molecular Formula | C19H21F6N4O7P |
| Molecular Weight | 562.356826543808 |
| Exact Mass | 562.105 |
| CAS # | 1256756-88-3 |
| Related CAS # | Retagliptin;1174122-54-3 |
| PubChem CID | 49820554 |
| Appearance | White to light yellow solid powder |
| Hydrogen Bond Donor Count | 4 |
| Hydrogen Bond Acceptor Count | 15 |
| Rotatable Bond Count | 6 |
| Heavy Atom Count | 37 |
| Complexity | 748 |
| Defined Atom Stereocenter Count | 1 |
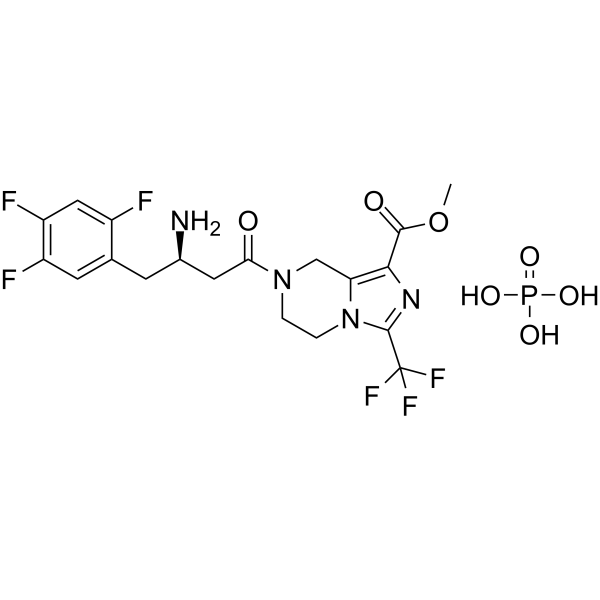
| SMILES | COC(=O)C1=C2CN(CCN2C(=N1)C(F)(F)F)C(=O)C[C@@H](CC3=CC(=C(C=C3F)F)F)N.OP(=O)(O)O |
| InChi Key | SFNHOWDAQMIJPX-HNCPQSOCSA-N |
| InChi Code | InChI=1S/C19H18F6N4O3.H3O4P/c1-32-17(31)16-14-8-28(2-3-29(14)18(27-16)19(23,24)25)15(30)6-10(26)4-9-5-12(21)13(22)7-11(9)20;1-5(2,3)4/h5,7,10H,2-4,6,8,26H2,1H3;(H3,1,2,3,4)/t10-;/m1./s1 |
| Chemical Name | methyl 7-[(3R)-3-amino-4-(2,4,5-trifluorophenyl)butanoyl]-3-(trifluoromethyl)-6,8-dihydro-5H-imidazo[1,5-a]pyrazine-1-carboxylate;phosphoric acid |
| HS Tariff Code | 2934.99.9001 |
| Storage |
Powder-20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month Note: Please store this product in a sealed and protected environment, avoid exposure to moisture. |
| Shipping Condition | Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs) |
Biological Activity
| Targets |
Dipeptidyl peptidase-4 (DPP-4) inhibitor |
| ln Vitro | Resagliptin is a family of chemicals used in the investigation of type 2 diabetes. Repagliptin inhibits the breakdown of GLP-1, hence enhancing the effects of incretin [1]. |
| ADME/Pharmacokinetics |
A single-dose, open-label study was conducted in 32 participants categorized by renal function (normal, mild, moderate, severe dysfunction, and end-stage renal disease (ESRD)) to evaluate the pharmacokinetics of Retagliptin Phosphate. All participants received a single 50 mg oral dose of the phosphate retagliptin tablet.[1] Plasma and urine concentrations of the prodrug phosphate retagliptin (SP2086) and its active metabolite retagliptin acid (SP2086 acid) were determined using validated liquid chromatography-tandem mass spectrometry (LC-MS/MS) methods.[1] Pharmacokinetic parameters were calculated from plasma concentration-time data using WinNolin 6.1 software.[1] For SP2086, the time to reach peak concentration (Tmax) increased with worsening renal function: 1.75±1.21 h (normal), 1.07±0.35 h (mild), 1.50±0.89 h (moderate), 1.67±2.16 h (severe), and 2.42±2.15 h (ESRD).[1] The apparent oral clearance (CL/F) of SP2086 decreased markedly with worsening renal function: 30.50±10.70 L/h (normal), 23.50±6.01 L/h (mild), 12.90±4.34 L/h (moderate), 6.70±1.55 L/h (severe), and 3.10±0.48 L/h (ESRD).[1] Both the prodrug (SP2086) and the active acid (SP2086 acid) showed an increase in peak concentration (Cmax) and area under the concentration-time curve (AUC), and a decrease in clearance with declining renal function.[1] The renal clearance (CLr) of the active metabolite SP2086 acid decreased with renal impairment: 289.0±73.7 mL/min (normal), 220.0±51.2 mL/min (mild), 105.0±64.5 mL/min (moderate), 54.5±7.6 mL/min (severe), and 13.5±7.8 mL/min (ESRD).[1] The 0-96 hour urine cumulative excretion percentage (Ae%) of SP2086 was low, ranging from 0.441% to 4.530% across groups. The Ae% of SP2086 acid was 74.2±14.6% in normal participants and decreased to 34.1±20.0% in ESRD patients.[1] Compared with participants with normal renal function, the AUC of SP2086 was 1.44, 2.20, and 2.83 times higher in patients with moderate, severe, and ESRD-level dysfunction, respectively. The AUC of SP2086 acid was 2.32, 4.39, and 9.28 times higher in the same groups, respectively.[1] |
| Toxicity/Toxicokinetics |
In a double-blind, phase III, placebo-controlled study in Chinese patients with type 2 diabetes, the proportions of patients who experienced adverse events were 27.78% for Retagliptin 100 mg once daily (qd), 20.55% for 50 mg twice daily (bid), and 15.97% for placebo.[2] The most common adverse events included upper respiratory tract infections, nasopharyngitis, and urinary tract infections.[2] Hypoglycemic events were reported: one patient on placebo, two on Retagliptin 100 mg qd, and five on Retagliptin 50 mg bid.[2] |
| References |
[1]. Pharmacokinetics of Phosphate Retagliptin Tabletin in Patients with Renal Dysfunction. Sichuan Da Xue Xue Bao Yi Xue Ban. 2018 Jan;49(1):74-80. [2]. An update on DPP-4 inhibitors in the management of type 2 diabetes. Expert Opin Emerg Drugs. 2016 Dec;21(4):409-419. |
| Additional Infomation |
Based on the observed increase in systemic exposure (AUC) with declining renal function, a dosage adjustment for Retagliptin Phosphate tablets is recommended.[1] The recommended dosage is 100 mg per day for patients with normal renal function and those with mild renal dysfunction, 50 mg per day for patients with moderate renal dysfunction, and 25 mg per day for patients with severe renal dysfunction. Retagliptin Phosphate tablets are not recommended for patients with end-stage renal disease (ESRD).[1] Retagliptin (SP-2086) is a novel DPP-4 inhibitor innovated in China and under development by Jiangsu Hengrui Medicine for the treatment of type 2 diabetes.[2] It is described as a competitive DPP-4 inhibitor and a tetrahydro-imidazo[1,5-a]pyrazine derivative, structurally similar to sitagliptin.[2] The company has completed two phase II clinical trials in China exploring the efficacy and safety of the drug as monotherapy and as an adjunct to metformin.[2] In a double-blind, phase III, placebo-controlled study, the efficacy and safety of Retagliptin were evaluated in Chinese patients with type 2 diabetes who had inadequate glycemic control with diet and exercise. After a 2-week placebo run-in period, 461 patients with HbA1c levels of 7-10.5% were randomized 1:1:1 to receive Retagliptin 100 mg qd, 50 mg bid, or placebo for 24 weeks.[2] Both Retagliptin groups showed significantly greater adjusted mean HbA1c decreases from baseline to week 24 compared with placebo (-1.07%, -1.20% vs. -0.34%; p<0.01), as well as reductions in fasting plasma glucose (-0.77 mmol/L, -1.03 mmol/L vs. -0.22 mmol/L; p<0.025).[2] A significantly greater proportion of patients achieved a therapeutic glycemic response (HbA1c <7.0%) with Retagliptin 100 mg qd (44.44%) and 50 mg bid (53.42%) versus placebo (26.39%; p<0.01).[2] An additional phase III trial with Retagliptin 50 mg qd or bid vs. placebo as add-on to metformin has also been conducted.[2] The company withdrew its application from the Chinese FDA in April 2016 but was expected to refile the application soon.[2] Retagliptin might be the first DPP-4 inhibitor launched in China by a domestic pharmaceutical company.[2] |
Solubility Data
| Solubility (In Vitro) | DMSO : ≥ 150 mg/mL (~266.73 mM) |
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 2.08 mg/mL (3.70 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 20.8 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 2.08 mg/mL (3.70 mM) (saturation unknown) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 20.8 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. Solubility in Formulation 3: ≥ 2.08 mg/mL (3.70 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 20.8 mg/mL clear DMSO stock solution to 900 μL of corn oil and mix evenly. (Please use freshly prepared in vivo formulations for optimal results.) |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 1.7782 mL | 8.8911 mL | 17.7822 mL | |
| 5 mM | 0.3556 mL | 1.7782 mL | 3.5564 mL | |
| 10 mM | 0.1778 mL | 0.8891 mL | 1.7782 mL |