Physicochemical Properties
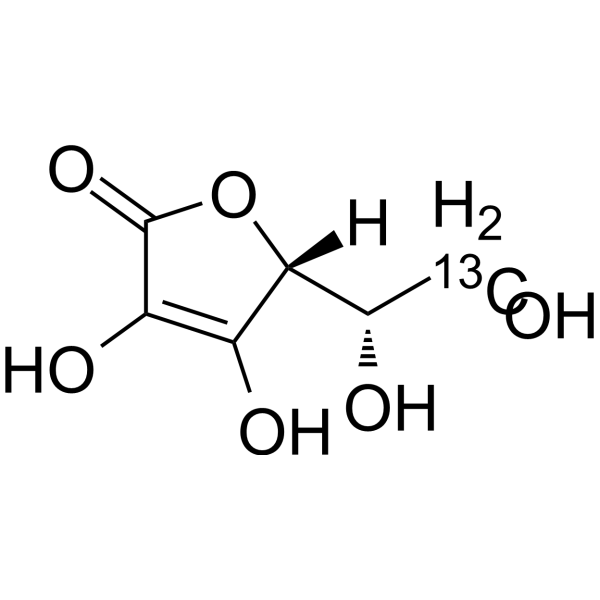
| Molecular Formula | C6H8O6 |
| Molecular Weight | 177.116777420044 |
| Exact Mass | 176.032 |
| CAS # | 149153-08-2 |
| Related CAS # | L-Ascorbic acid;50-81-7 |
| PubChem CID | 54676860 |
| Appearance | Typically exists as solid at room temperature |
| LogP | -1.6 |
| Hydrogen Bond Donor Count | 4 |
| Hydrogen Bond Acceptor Count | 6 |
| Rotatable Bond Count | 2 |
| Heavy Atom Count | 12 |
| Complexity | 232 |
| Defined Atom Stereocenter Count | 0 |
| InChi Key | CIWBSHSKHKDKBQ-UHFFFAOYSA-N |
| InChi Code | InChI=1S/C6H8O6/c7-1-2(8)5-3(9)4(10)6(11)12-5/h2,5,7-10H,1H2 |
| Chemical Name | 2-(1,2-dihydroxyethyl)-3,4-dihydroxy-2H-furan-5-one |
| HS Tariff Code | 2934.99.9001 |
| Storage |
Powder-20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month |
| Shipping Condition | Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs) |
Biological Activity
| ln Vitro | Drug compounds have included stable heavy isotopes of carbon, hydrogen, and other elements, mostly as quantitative tracers while the drugs were being developed. Because deuteration may have an effect on a drug's pharmacokinetics and metabolic properties, it is a cause for concern [1]. |
| ADME/Pharmacokinetics |
Absorption, Distribution and Excretion The efficiency of absorption depends on the salt form, the amount administered, the dosing regimen and the size of iron stores. Subjects with normal iron stores absorb 10% to 35% of an iron dose. Those who are iron deficient may absorb up to 95% of an iron dose. |
| Toxicity/Toxicokinetics |
Effects During Pregnancy and Lactation ◉ Summary of Use during Lactation Vitamin C is a normal component of human milk and is a key milk antioxidant. The recommended vitamin C intake in lactating women is 120 mg daily, and for infants aged 6 months or less is 40 mg daily. High daily doses up to 1000 mg increase milk levels, but not enough to cause a health concern for the breastfed infant and is not a reason to discontinue breastfeeding. Nursing mothers may need to supplement their diet to achieve the recommended intake or to correct a known deficiency. Maternal doses of vitamin C in prenatal vitamins at or near the recommended intake do not alter milk levels. Freezing (-20 degrees C) freshly expressed mature milk from hospitalized mothers of term and preterm infants does not change milk vitamin C levels for at least 3 months of freezer storage. After 6 to 12 months of freezing (-20 degrees C), vitamin C levels can decrease by 15 to 30%. Storage at -80 degrees C preserves vitamin C levels for up to 8 months, with 15% loss by 12 months. ◉ Effects in Breastfed Infants Sixty healthy lactating women between 1 and 6 months postpartum exclusively breastfeeding their infants were given vitamin C 500 mg plus vitamin E 100 IU once daily for 30 days, or no supplementation. Infants of supplemented mothers had increased biochemical markers of antioxidant activity in their urine. Clinical outcomes were not reported. Eighteen preterm infants, seven of whom were less than 32 weeks gestational age, who were fed pooled, Holder-pasteurized donor milk beginning during the first three days of life had their average blood plasma ascorbic acid concentrations decrease from 15.5 mg/L at birth to 5.4 mg/L by 1 week of age, and to 4.1 mg/L by 3 weeks of age. The authors described the 1- and 3-week levels as subtherapeutic (<6 mg/L) and indicative of inadequate intake, potentially jeopardizing postnatal growth potential. Although this study was conducted before advances in the provision of parenteral nutrition and enteral milk fortification for preterm infants, contemporary studies suggest that inadequate vitamin C intake from pooled, pasteurized donor milk may be a potential health problem for preterm infants receiving donor milk. ◉ Effects on Lactation and Breastmilk Relevant published information was not found as of the revision date. |
| References |
[1]. Impact of Deuterium Substitution on the Pharmacokinetics of Pharmaceuticals. Ann Pharmacother. 2019 Feb;53(2):211-216. [2]. Vitamin C as an antioxidant: evaluation of its role in disease prevention. J Am Coll Nutr. 2003 Feb;22(1):18-35. |
| Additional Infomation |
D-erythro-Hex-2-enonic acid, gamma-lactone has been reported in Pisum sativum and Hippophae with data available. A six carbon compound related to glucose. It is found naturally in citrus fruits and many vegetables. Ascorbic acid is an essential nutrient in human diets, and necessary to maintain connective tissue and bone. Its biologically active form, vitamin C, functions as a reducing agent and coenzyme in several metabolic pathways. Vitamin C is considered an antioxidant. See also: Ascorbate (annotation moved to); D-ascorbic acid (annotation moved to); Ascorbic Acid (annotation moved to) ... View More ... Drug Indication Used in preventing and treating iron-deficiency anemia. Mechanism of Action Iron is necessary for the production of hemoglobin. Iron-deficiency can lead to decreased production of hemoglobin and a microcytic, hypochromic anemia. |
Solubility Data
| Solubility (In Vitro) | May dissolve in DMSO (in most cases), if not, try other solvents such as H2O, Ethanol, or DMF with a minute amount of products to avoid loss of samples |
| Solubility (In Vivo) |
Note: Listed below are some common formulations that may be used to formulate products with low water solubility (e.g. < 1 mg/mL), you may test these formulations using a minute amount of products to avoid loss of samples. Injection Formulations (e.g. IP/IV/IM/SC) Injection Formulation 1: DMSO : Tween 80: Saline = 10 : 5 : 85 (i.e. 100 μL DMSO stock solution → 50 μL Tween 80 → 850 μL Saline) *Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH ₂ O to obtain a clear solution. Injection Formulation 2: DMSO : PEG300 :Tween 80 : Saline = 10 : 40 : 5 : 45 (i.e. 100 μL DMSO → 400 μLPEG300 → 50 μL Tween 80 → 450 μL Saline) Injection Formulation 3: DMSO : Corn oil = 10 : 90 (i.e. 100 μL DMSO → 900 μL Corn oil) Example: Take the Injection Formulation 3 (DMSO : Corn oil = 10 : 90) as an example, if 1 mL of 2.5 mg/mL working solution is to be prepared, you can take 100 μL 25 mg/mL DMSO stock solution and add to 900 μL corn oil, mix well to obtain a clear or suspension solution (2.5 mg/mL, ready for use in animals). Injection Formulation 4: DMSO : 20% SBE-β-CD in saline = 10 : 90 [i.e. 100 μL DMSO → 900 μL (20% SBE-β-CD in saline)] *Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. Injection Formulation 5: 2-Hydroxypropyl-β-cyclodextrin : Saline = 50 : 50 (i.e. 500 μL 2-Hydroxypropyl-β-cyclodextrin → 500 μL Saline) Injection Formulation 6: DMSO : PEG300 : castor oil : Saline = 5 : 10 : 20 : 65 (i.e. 50 μL DMSO → 100 μLPEG300 → 200 μL castor oil → 650 μL Saline) Injection Formulation 7: Ethanol : Cremophor : Saline = 10: 10 : 80 (i.e. 100 μL Ethanol → 100 μL Cremophor → 800 μL Saline) Injection Formulation 8: Dissolve in Cremophor/Ethanol (50 : 50), then diluted by Saline Injection Formulation 9: EtOH : Corn oil = 10 : 90 (i.e. 100 μL EtOH → 900 μL Corn oil) Injection Formulation 10: EtOH : PEG300:Tween 80 : Saline = 10 : 40 : 5 : 45 (i.e. 100 μL EtOH → 400 μLPEG300 → 50 μL Tween 80 → 450 μL Saline) Oral Formulations Oral Formulation 1: Suspend in 0.5% CMC Na (carboxymethylcellulose sodium) Oral Formulation 2: Suspend in 0.5% Carboxymethyl cellulose Example: Take the Oral Formulation 1 (Suspend in 0.5% CMC Na) as an example, if 100 mL of 2.5 mg/mL working solution is to be prepared, you can first prepare 0.5% CMC Na solution by measuring 0.5 g CMC Na and dissolve it in 100 mL ddH2O to obtain a clear solution; then add 250 mg of the product to 100 mL 0.5% CMC Na solution, to make the suspension solution (2.5 mg/mL, ready for use in animals). Oral Formulation 3: Dissolved in PEG400 Oral Formulation 4: Suspend in 0.2% Carboxymethyl cellulose Oral Formulation 5: Dissolve in 0.25% Tween 80 and 0.5% Carboxymethyl cellulose Oral Formulation 6: Mixing with food powders Note: Please be aware that the above formulations are for reference only. InvivoChem strongly recommends customers to read literature methods/protocols carefully before determining which formulation you should use for in vivo studies, as different compounds have different solubility properties and have to be formulated differently. (Please use freshly prepared in vivo formulations for optimal results.) |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 5.6459 mL | 28.2294 mL | 56.4589 mL | |
| 5 mM | 1.1292 mL | 5.6459 mL | 11.2918 mL | |
| 10 mM | 0.5646 mL | 2.8229 mL | 5.6459 mL |