Physicochemical Properties
| Molecular Formula | C27H29O6F3S |
| Molecular Weight | 538.57576 |
| Exact Mass | 538.163 |
| Elemental Analysis | C, 60.21; H, 5.43; F, 10.58; O, 17.82; S, 5.95 |
| CAS # | 397864-44-7 |
| Related CAS # | Fluticasone (propionate);80474-14-2;Fluticasone furoate-d3 |
| PubChem CID | 9854489 |
| Appearance | White to off-white solid powder |
| Density | 1.4±0.1 g/cm3 |
| Boiling Point | 625.2±55.0 °C at 760 mmHg |
| Melting Point | 250-252 |
| Flash Point | 331.9±31.5 °C |
| Vapour Pressure | 0.0±1.9 mmHg at 25°C |
| Index of Refraction | 1.584 |
| LogP | 4.01 |
| Hydrogen Bond Donor Count | 1 |
| Hydrogen Bond Acceptor Count | 10 |
| Rotatable Bond Count | 6 |
| Heavy Atom Count | 37 |
| Complexity | 1080 |
| Defined Atom Stereocenter Count | 9 |
| SMILES | C[C@@H]1C[C@H]2[C@@H]3C[C@@H](C4=CC(=O)C=C[C@]4(C)[C@]3([C@H](C[C@]2(C)[C@]1(C(=O)SCF)OC(=O)C5=CC=CO5)O)F)F |
| InChi Key | XTULMSXFIHGYFS-VLSRWLAYSA-N |
| InChi Code | InChI=1S/C27H29F3O6S/c1-14-9-16-17-11-19(29)18-10-15(31)6-7-24(18,2)26(17,30)21(32)12-25(16,3)27(14,23(34)37-13-28)36-22(33)20-5-4-8-35-20/h4-8,10,14,16-17,19,21,32H,9,11-13H2,1-3H3/t14-,16+,17+,19+,21+,24+,25+,26+,27+/m1/s1 |
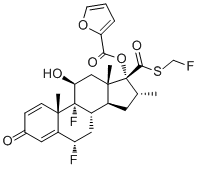
| Chemical Name | (6S,8S,9R,10S,11S,13S,14S,16R,17R)-6,9-difluoro-17-(((fluoromethyl)thio)carbonyl)-11-hydroxy-10,13,16-trimethyl-3-oxo-6,7,8,9,10,11,12,13,14,15,16,17-dodecahydro-3H-cyclopenta[a]phenanthren-17-yl furan-2-carboxylate |
| Synonyms | Avamys; Veramyst; Fluticasone furoate; 397864-44-7; Veramyst; Avamys; Allermist; Furamist; Arnuity Ellipta; Alisade; Allermist |
| HS Tariff Code | 2934.99.9001 |
| Storage |
Powder-20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month |
| Shipping Condition | Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs) |
Biological Activity
| Targets |
Corticosteroid (Kd = 0.3 nM) Glucocorticoid receptor [1] |
| ln Vitro |
By means of a metered atomizing spray pump, fluticasone furoate is applied locally to the nasal mucosa as an aqueous suspension of micronized fluticasone furoate in the form of a nasal spray [1]. Inappropriate stimulation of cultured human lung epithelial cells can be efficiently prevented by fluticasone furoate [1]. In vitro studies showed that fluticasone furoate displayed high selectivity for the glucocorticoid receptor and had greater relative receptor affinity (2989, relative to dexamethasone) compared to other corticosteroids such as mometasone furoate, fluticasone propionate, beclomethasone-17-monopropionate, and budesonide. [1] Fluticasone furoate exhibited greater potency than other corticosteroids in inhibiting tumor necrosis factor synthesis and action in vitro. [1] It was also more potent in preventing damage to cultured human lung epithelial cells induced by different stimuli. [1] |
| ln Vivo |
In vitro, fluticasone furoate is 99.4% bound to oxidants, and additional research has demonstrated that the drug's effects are wide-ranging when it is absorbed. Because only unbound oxidant medications are able to act at the receptor site, proteins are extremely important. Fluticasone furoate is primarily cleared from the body by cytochrome P450 isoenzyme (CYP) 3A4, which processes the medication and transforms it into 17β-sulfamate (M10), a drug that effectively binds to the hypoglycemic hormone receptor. ..Only a small amount of fluticasone furoate is excreted in the feces, which is where it is mostly excreted [1]. In multiple double-blind, placebo-controlled clinical trials involving patients with seasonal or perennial allergic rhinitis, once-daily intranasal fluticasone furoate (at a dose of 110 µg for adults/adolescents) was superior to placebo in reducing both nasal and ocular symptoms. Significant improvements were observed in reflective and instantaneous total nasal symptom scores (rTNSS, iTNSS) and total ocular symptom scores (rTOSS, iTOSS). [1] In a dose-ranging study in seasonal allergic rhinitis patients, the 110 µg dose provided the optimal benefit-risk ratio. A statistically significant difference compared to placebo was first noted at 24 hours after the first dose for instantaneous total nasal symptom score. [1] A study assessing short-term lower-leg growth rate in children with allergic rhinitis treated with fluticasone furoate nasal spray found no effect on growth rate, as measured by knemometry. [1] Long-term (12-month) treatment with fluticasone furoate in adults and adolescents was well-tolerated, with no evidence of clinically relevant systemic corticosteroid exposure. [1] |
| Enzyme Assay |
Fluticasone furonate has high receptor affinity, with low equilibrium dissociation constant (kd = 0.3 nmol/L) and with greater relative receptor affinity (2989) than mometasone furoate (2244), fluticasone propionate (1775), beclomethasone-17-monopropionate (1345), ciclesonide active principle (1212), and budesonide (855)[1]. Some in vitro studies showed that FF displayed greater potency than other corticosteroids in inhibiting tumor necrosis factor synthesis and action. It was also more potent in preventing damage to cultured human lung epithelial cells by different stimulus. Experimental studies demonstrated more potent and faster anti-inflammatory activity of FF than fluticasone propionate[1]. |
| Cell Assay | Asthma is a complex disease with diverse clinical manifestations ranging from mild to severe. Despite existing guidelines for asthma recognition and treatment, still a proportion of patients stay uncontrolled. Combinational therapy which comprises inhaled corticosteroids (ICS) and a long acting B2 adrenreceptor agonist (LABA) has been suggested to control asthma. In this study T-bet expression was attested in CD4 T cells treated with Fluticasone Furoate (FF), Vilanterol (V) and FF/V combination in severe asthmatic patients compared to patients with moderate asthma and healthy controls using Immunocytochemistry (ICC). First, CD4 T cells were isolated from PBMCs of 12 patients and controls using CD4 T cell isolation kit. Subsequently, isolated CD4 T cells were cultured with FF, V and FF/V for 1 h. To accomplish ICC, cells were incubated with anti-T-bet antibody, and then stained with HRP-bound secondary antibody. T-bet expression was evaluated using light microscopy. Statistical analyses were performed using R 3.5.2 software and visualized by ggplot2 3.1.0 package. Significant increasing in T-bet expression was seen in CD4 T cells from patients with moderate asthma treated with FF and FF/V. Suggesting conclusion would be distinct mechanisms responsible for severe asthma and moderate asthma in the patients and the needs for novel therapies. Further molecular studies in different asthma phenotypes would be instructive for asthma treatment [2]. |
| Animal Protocol |
Allergic rhinitis (AR) is a prevalent disease with great morbidity and significant societal and economic burden. Intranasal corticosteroids are recommended as first-line therapy for patients with moderate-to-severe disease, especially when nasal congestion is a major component of symptoms. To compare the efficacy and safety profile of different available intranasal corticosteroids for the treatment of AR, it is important to understand their different structures and pharmacokinetic and pharmacodynamic properties. Knowledge of these drugs has increased tremendously over the last decade. Studies have elucidated mechanisms of action, pharmacologic properties, and the clinical impact of these drugs in allergic respiratory diseases. Although the existing intranasal corticosteroids are already highly efficient, the introduction of further improved formulations with a better efficacy/safety profile is always desired. Fluticasone furoate nasal spray is a new topical corticosteroid, with enhanced-affinity and a unique side-actuated delivery device. As it has high topical potency and low potential for systemic effects, it is a good candidate for rhinitis treatment [1]. After single- and multiple-dose intranasal administration, plasma fluticasone furoate concentrations are below the lower limit of quantification in most patients (Allen et al 2007; Hughes et al 2007; Martin 2007). One study showed that only 2% of samples from patients receiving 110 μg of FF had quantifiable plasma drug concentrations (Martin 2007). Systemic bioavailability is determined by the sum of 2 components, including the portion of the drug that is absorbed via the nasal mucosa plus the portion that is swallowed. The last one is the major route for circulation, what makes the first-pass hepatic metabolism after drug absorption in the gastrointestinal tract very important[1]. |
| ADME/Pharmacokinetics |
Absorption, Distribution and Excretion Fluticasone furoate plasma levels may not predict therapeutic effect. Peak plasma concentrations are reached within 0.5 to 1 hour. Absolute bioavailability of fluticasone furoate when administrated by inhalation was 13.9%, primarily due to absorption of the inhaled portion of the dose delivered to the lung. Oral bioavailability from the swallowed portion of the dose is low (approximately 1.3%) due to extensive first-pass metabolism. Systemic exposure (AUC) in subjects with asthma was 26% lower than observed in healthy subjects. Following repeat dosing of inhaled fluticasone furoate, steady state was achieved within 6 days with up to 2.6-fold accumulation. Intranasal exposure of fluticasone furoate also results in patients swallowing a larger portion of the dose. Following intravenous dosing with radiolabeled fluticasone furoate, mass balance showed 90% of radiolabel in the feces and 2% in the urine. Following oral dosing, radiolabel recovered in feces was 101% of the total dose, and that in urine was approximately 1% of the total dose. Following intravenous administration to healthy subjects, the mean volume of distribution at steady state was 661 L. A study of 24 healthy Caucasian males showed a volume of distribution at steady state of 704L following intravenous administration. Following intravenous administration to healthy subjects, fluticasone furoate was cleared from systemic circulation principally by hepatic metabolism via CYP3A4 with a total plasma clearance of 65.4 L/hr. A study of 24 healthy Caucasian males also showed a clearance of 71.8L/h following intravenous administration. Metabolism / Metabolites Fluticasone furoate is cleared from systemic circulation principally by hepatic metabolism via CYP3A4 to metabolites with significantly reduced corticosteroid activity. There was no in vivo evidence for cleavage of the furoate moiety resulting in the formation of fluticasone. Fluticasone furoate is also hydrolyzed at the FIVE-S-fluoromethyl carbothioate group, forming an inactive metabolite. Biological Half-Life Following repeat-dose inhaled administration, the plasma elimination phase half-life averaged 24 hours. A study of 24 healthy Caucasian males showed a half-life of 13.6 hours following intravenous administration and 17.3-23.9 hours following inhalation. After single- and multiple-dose intranasal administration, plasma concentrations of fluticasone furoate are generally below the lower limit of quantification in most patients. [1] The average absolute bioavailability after intranasal administration (880 µg every 8 hours for 10 doses) in healthy volunteers was 0.5%. [1] The oral bioavailability after a single 2 mg oral dose is 1.26%. [1] The elimination half-life after a single intravenous dose is 15.1 hours. [1] In vitro, fluticasone furoate is 99.4% bound to plasma proteins. [1] The drug undergoes extensive first-pass metabolism, primarily in the liver via the cytochrome P450 isozyme CYP3A4, which hydrolyzes it to the 17β-carboxylic acid metabolite (M10), a metabolite with low glucocorticoid receptor agonist potency. [1] Fluticasone furoate is excreted mainly in the feces, with only minor amounts appearing in the urine. [1] |
| Toxicity/Toxicokinetics |
Protein Binding Fluticasone furoate is >99% protein bound in serum and may be as high as 99.6%, predominantly to albumin (96%) and α1-acid glycoprotein (90%). In pooled analyses of clinical trials, the overall incidence of adverse events with intranasal fluticasone furoate was similar to that with placebo. [1] The most common adverse events (incidence ≥1% in adolescents/adults or ≥3% in children, and higher than placebo) included: headache, epistaxis (nosebleed), nasopharyngitis, pyrexia, pharyngolaryngeal pain, nasal ulceration, cough, and back pain. [1] Epistaxis was the only adverse event occurring more frequently and with greater severity among fluticasone furoate recipients compared to placebo, particularly during long-term (12-month) therapy. [1] There is a caution regarding co-administration with potent CYP3A4 inhibitors (e.g., ketoconazole, ritonavir), as this may increase systemic exposure to fluticasone furoate and potentially increase the risk of systemic adverse effects. [1] |
| References |
[1]. Fluticasone furoate nasal spray in the treatment of allergic rhinitis. Ther Clin Risk Manag. 2008 Apr;4(2):465-72. [2]. Asthma phenotypes and T-bet protein expression in cells treated with Fluticasone Furoate/Vilanterol. Pulm Pharmacol Ther. 2020 Feb;60:101886. |
| Additional Infomation |
Fluticasone furoate is a trifluorinated corticosteroid that consists of 6alpha,9-difluoro-11beta,17alpha-dihydroxy-17beta-{[(fluoromethyl)sulfanyl]carbonyl}-16-methyl-3-oxoandrosta-1,4-diene bearing a 2-furoyl substituent at position 17. Used in combination with vilanterol trifenate for treatment of bronchospasm associated with chronic obstructive pulmonary disease. It has a role as an anti-allergic agent, a prodrug and an anti-asthmatic drug. It is an 11beta-hydroxy steroid, a corticosteroid, a fluorinated steroid, a steroid ester, a 2-furoate ester, a thioester and a 3-oxo-Delta(1),Delta(4)-steroid. It is functionally related to a fluticasone. It derives from a hydride of an androstane. Fluticasone furoate is a synthetic glucocorticoid available as an inhaler and nasal spray for various inflammatory indications. Fluticasone furoate was first approved in 2007. Fluticasone Furoate is the furoate salt form of fluticasone, a synthetic trifluorinated glucocorticoid receptor agonist with anti-allergic, anti-inflammatory and anti-pruritic effects. Upon administration, fluticasone binds to and activates glucocorticoid receptor, resulting in the activation of lipocortin. Lipocortin, in turn, inhibits cytosolic phospholipase A2 and the cascade of reactions involved in the synthesis of inflammatory mediators, such as prostaglandins and leukotrienes. Secondly, mitogen-activated protein kinase (MAPK) phosphatase 1 is induced, which leads to dephosphorylation and inactivation of Jun N-terminal kinase and directly inhibits c-Jun mediated transcription. Finally, transcriptional activity of nuclear factor (NF)-kappa-B is blocked, thereby inhibiting the transcription of cyclooxygenase 2 (COX-2), which is essential for prostaglandin production. See also: Fluticasone (has active moiety); Fluticasone furoate; vilanterol trifenatate (component of) ... View More ... Drug Indication Fluticasone furoate is indicated for once-daily maintenance (i.e. prophylactic) treatment of asthma in patients ≥5 years old. Fluticasone furoate is available in two combination medications - one in combination with [vilanterol] and one in combination with both vilanterol and [umeclidinium]- which are both indicated for the management of chronic obstructive pulmonary disease (COPD) and for the treatment of asthma in patients ≥18 years old for the vilanterol-umeclidinium-fluticasone product and ≥5 years old for the vilanterol-fluticasone product. Fluticasone furoate is available over the counter as a nasal spray for the symptomatic treatment of hay fever and other upper respiratory allergies in patients ≥2 years old. FDA Label Adults, adolescents (12 years and over) and children (6-11 years). Avamys is indicated for the treatment of the symptoms of allergic rhinitis. Adults, adolescents (12 years and over) and children (6 - 11 years). Alisade is indicated for the treatment of the symptoms of allergic rhinitis. Mechanism of Action Fluticasone furoate has been shown in vitro to exhibit a binding affinity for the human glucocorticoid receptor that is approximately 29.9 times that of dexamethasone and 1.7 times that of fluticasone propionate. The clinical relevance of these findings is unknown. The precise mechanism through which fluticasone furoate affects asthma symptoms is not known. Inflammation is an important component in the pathogenesis of asthma. Corticosteroids have been shown to have a wide range of actions on multiple cell types (e.g., mast cells, eosinophils, neutrophils, macrophages, lymphocytes) and mediators (e.g., histamine, eicosanoids, leukotrienes, cytokines) involved in inflammation. Specific effects of fluticasone furoate demonstrated in in vitro and in vivo models included activation of the glucocorticoid response element, inhibition of pro-inflammatory transcription factors such as NFkB, and inhibition of antigen-induced lung eosinophilia in sensitized rats. These anti-inflammatory actions of corticosteroids may contribute to their efficacy. Fluticasone furoate is a synthetic, trifluorinated, topical glucocorticoid with enhanced receptor affinity and potent anti-inflammatory activity. [1] It is formulated as an aqueous suspension nasal spray for topical administration to the nasal mucosa. Each actuation delivers 27.5 µg of fluticasone furoate in a 50 µL volume. [1] The formulation contains excipients/preservatives including benzalkonium chloride (0.015% w/w), dextrose anhydrous, edetate disodium, microcrystalline cellulose, carboxymethylcellulose sodium, polysorbate 80, and purified water. [1] It is administered via a unique, side-actuated nasal spray device designed to minimize dose variation and throat rundown. [1] The recommended starting dose is 55 µg once daily for children and 110 µg once daily for adults and adolescents. [1] It is indicated for the treatment of allergic rhinitis symptoms in patients aged 2 years and older. [1] The drug acts by binding to intracellular glucocorticoid receptors, leading to inhibition of the production of various cytokines, chemokines, enzymes, and cell adhesion molecules involved in inflammation. [1] The low systemic bioavailability and high plasma protein binding contribute to its minimal systemic adverse effects. [1] |
Solubility Data
| Solubility (In Vitro) | DMSO : ~100 mg/mL (~185.67 mM) |
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 2.5 mg/mL (4.64 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 2.5 mg/mL (4.64 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 900 μL of corn oil and mix evenly. (Please use freshly prepared in vivo formulations for optimal results.) |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 1.8567 mL | 9.2837 mL | 18.5673 mL | |
| 5 mM | 0.3713 mL | 1.8567 mL | 3.7135 mL | |
| 10 mM | 0.1857 mL | 0.9284 mL | 1.8567 mL |