Physicochemical Properties
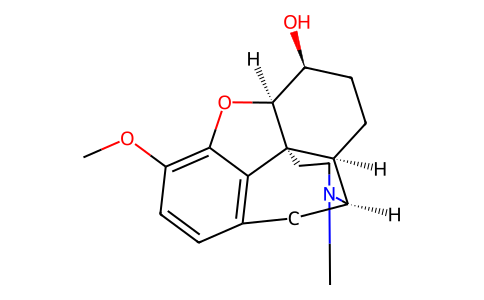
| Molecular Formula | C18H23NO3 |
| Molecular Weight | 301.38012 |
| Exact Mass | 301.167 |
| CAS # | 125-28-0 |
| PubChem CID | 5284543 |
| Appearance | Typically exists as solid at room temperature |
| LogP | 2.2 |
| Hydrogen Bond Donor Count | 1 |
| Hydrogen Bond Acceptor Count | 4 |
| Rotatable Bond Count | 1 |
| Heavy Atom Count | 22 |
| Complexity | 471 |
| Defined Atom Stereocenter Count | 5 |
| SMILES | CN1CC[C@]23[C@@H]4[C@H]1CC5=C2C(=C(C=C5)OC)O[C@H]3[C@H](CC4)O |
| InChi Key | RBOXVHNMENFORY-DNJOTXNNSA-N |
| InChi Code | InChI=1S/C18H23NO3/c1-19-8-7-18-11-4-5-13(20)17(18)22-16-14(21-2)6-3-10(15(16)18)9-12(11)19/h3,6,11-13,17,20H,4-5,7-9H2,1-2H3/t11-,12+,13-,17-,18-/m0/s1 |
| Chemical Name | (4R,4aR,7S,7aR,12bS)-9-methoxy-3-methyl-2,4,4a,5,6,7,7a,13-octahydro-1H-4,12-methanobenzofuro[3,2-e]isoquinolin-7-ol |
| Synonyms | Hydrocodeine; Cohydrin; Dihydrocodeine |
| HS Tariff Code | 2934.99.9001 |
| Storage |
Powder-20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month |
| Shipping Condition | Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs) |
Biological Activity
| ADME/Pharmacokinetics |
Absorption, Distribution and Excretion Bioavailability is low (approximately 20%) if administered orally. This may be due to poor gastrointestinal absorption. It is also likely due to pre-systemic metabolism by the liver and intestinal wall. [2] The AUCs after oral and intravenous administration are similar (3203ug/l/h and 3401ug/l/h, respectively). [2] Time to peak values are 1.6 and 1.8hours for a 30mg and 60mg dose, respectively. The concentrations achieved were 71.8 ug/1 and 146 ug/1, respectively. [2] Renal elimination and urinary excretion. [1] The disposition of dihydrocodeine is described as a two compartment model. [2] Plasma clearance is approximately 300ml/min. [2] The pharmacokinetics of dihydrocodeine and active metabolite dihydromorphine have been reported to be linear. [1] The decline in plasma dihydrocodeine concentrations after intravenous administration has been described as bi-exponential, with a sleep decline in the initial 2h following administration, followed by a mono-exponential decline thereafter. Clearance was not dose dependent. [2] Metabolism / Metabolites Metabolized in the liver by CYP 2D6 into an active metabolite, dihydromorphine, and by CYP 3A4 into secondary primary metabolite, nordihydrocodeine. A third primary metabolite is dihydrocodeine-6-glucuronide. [1] The time for mean peak concentration in acid metabolites is 1.76h and 1.98h for a 30 and 60mg dose, respectively. The concentrations achieved were 563 ug/1 and 1476 ug/1, respectively. [2] Dihydrocodeine has known human metabolites that include Desmethyl dihydrocodeine and Paramorfan. Biological Half-Life 4h |
| Toxicity/Toxicokinetics |
Effects During Pregnancy and Lactation ◉ Summary of Use during Lactation Maternal use of oral opioids during breastfeeding can cause infant drowsiness, which may progress to rare but severe central nervous system depression. Like codeine, pharmacogenetics probably plays a role in the extent of central nervous system depression with dihydrocodeine. Newborn infants seem to be particularly sensitive to the effects of even small dosages of narcotic analgesics. Dihydrocodeine possibly caused severe respiratory depression in one newborn infant whose mother was taking the drug for cough. If dihydrocodeine is required by the mother of a newborn, it is not a reason to discontinue breastfeeding; however, once the mother's milk comes in, it is best to provide pain control with a nonnarcotic analgesic and limit maternal intake of dihydrocodeine to 2 to 3 days at a low dosage with close infant monitoring. If the baby shows signs of increased sleepiness (more than usual), difficulty breastfeeding, breathing difficulties, or limpness, a physician should be contacted immediately. Because there is little published experience with dihydrocodeine during breastfeeding, an alternate drug may be preferred, especially while nursing a newborn or preterm infant. ◉ Effects in Breastfed Infants A woman began taking dihydrocodeine drops for cough twice daily (5.28 mg) beginning on the first day postpartum. One day later, her breastfed infant was difficult to arouse and was not breastfeeding well. The infant had bradycardia, hypoglycemia, and an oxygen saturation of 85%. After 24 hours in the hospital, all symptoms resolved. The symptoms were possibly caused by dihydrocodeine in milk. ◉ Effects on Lactation and Breastmilk Narcotics can increase serum prolactin. However, the prolactin level in a mother with established lactation may not affect her ability to breastfeed. |
| Additional Infomation |
Dihydrocodeine is a morphinane alkaloid. Dihydrocodeine is a DEA Schedule II controlled substance. Substances in the DEA Schedule II have a high potential for abuse which may lead to severe psychological or physical dependence. It is a Opiates substance. Dihydrocodeine is an opioid analgesic used as an alternative or adjunct to codeine to treat moderate to severe pain, severe dyspnea, and cough. It is semi-synthetic, and was developed in Germany in 1908 during an international search to find a more effective antitussive agent to help reduce the spread of airborne infectious diseases such as tuburculosis. It was marketed in 1911. Dihydrocodeine is an Opioid Agonist. The mechanism of action of dihydrocodeine is as a Full Opioid Agonist. Dihydrocodeine has been reported in Papaver somniferum with data available. Drug Indication Dihydrocodeine is used for the treatment of moderate to severe pain, including post-operative and dental pain [2]. It can also be used to treat chronic pain [1], breathlessness and coughing. In heroin addicts, dihydrocodeine has been used as a substitute drug, in doses up to 2500mg/day to treat addiction. [http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2014322/] Mechanism of Action Dihydrocodeine is metabolized to dihydromorphine -- a highly active metabolite with a high affinity for mu opioid receptors. [3] Pharmacodynamics Possible opioid related side effects include, but are not limited to, drowsiness, nausea, headache, dry mouth, constipation, difficulty passing urine, and mild euphoria. |
Solubility Data
| Solubility (In Vitro) | May dissolve in DMSO (in most cases), if not, try other solvents such as H2O, Ethanol, or DMF with a minute amount of products to avoid loss of samples |
| Solubility (In Vivo) |
Note: Listed below are some common formulations that may be used to formulate products with low water solubility (e.g. < 1 mg/mL), you may test these formulations using a minute amount of products to avoid loss of samples. Injection Formulations (e.g. IP/IV/IM/SC) Injection Formulation 1: DMSO : Tween 80: Saline = 10 : 5 : 85 (i.e. 100 μL DMSO stock solution → 50 μL Tween 80 → 850 μL Saline) *Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH ₂ O to obtain a clear solution. Injection Formulation 2: DMSO : PEG300 :Tween 80 : Saline = 10 : 40 : 5 : 45 (i.e. 100 μL DMSO → 400 μLPEG300 → 50 μL Tween 80 → 450 μL Saline) Injection Formulation 3: DMSO : Corn oil = 10 : 90 (i.e. 100 μL DMSO → 900 μL Corn oil) Example: Take the Injection Formulation 3 (DMSO : Corn oil = 10 : 90) as an example, if 1 mL of 2.5 mg/mL working solution is to be prepared, you can take 100 μL 25 mg/mL DMSO stock solution and add to 900 μL corn oil, mix well to obtain a clear or suspension solution (2.5 mg/mL, ready for use in animals). Injection Formulation 4: DMSO : 20% SBE-β-CD in saline = 10 : 90 [i.e. 100 μL DMSO → 900 μL (20% SBE-β-CD in saline)] *Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. Injection Formulation 5: 2-Hydroxypropyl-β-cyclodextrin : Saline = 50 : 50 (i.e. 500 μL 2-Hydroxypropyl-β-cyclodextrin → 500 μL Saline) Injection Formulation 6: DMSO : PEG300 : castor oil : Saline = 5 : 10 : 20 : 65 (i.e. 50 μL DMSO → 100 μLPEG300 → 200 μL castor oil → 650 μL Saline) Injection Formulation 7: Ethanol : Cremophor : Saline = 10: 10 : 80 (i.e. 100 μL Ethanol → 100 μL Cremophor → 800 μL Saline) Injection Formulation 8: Dissolve in Cremophor/Ethanol (50 : 50), then diluted by Saline Injection Formulation 9: EtOH : Corn oil = 10 : 90 (i.e. 100 μL EtOH → 900 μL Corn oil) Injection Formulation 10: EtOH : PEG300:Tween 80 : Saline = 10 : 40 : 5 : 45 (i.e. 100 μL EtOH → 400 μLPEG300 → 50 μL Tween 80 → 450 μL Saline) Oral Formulations Oral Formulation 1: Suspend in 0.5% CMC Na (carboxymethylcellulose sodium) Oral Formulation 2: Suspend in 0.5% Carboxymethyl cellulose Example: Take the Oral Formulation 1 (Suspend in 0.5% CMC Na) as an example, if 100 mL of 2.5 mg/mL working solution is to be prepared, you can first prepare 0.5% CMC Na solution by measuring 0.5 g CMC Na and dissolve it in 100 mL ddH2O to obtain a clear solution; then add 250 mg of the product to 100 mL 0.5% CMC Na solution, to make the suspension solution (2.5 mg/mL, ready for use in animals). Oral Formulation 3: Dissolved in PEG400 Oral Formulation 4: Suspend in 0.2% Carboxymethyl cellulose Oral Formulation 5: Dissolve in 0.25% Tween 80 and 0.5% Carboxymethyl cellulose Oral Formulation 6: Mixing with food powders Note: Please be aware that the above formulations are for reference only. InvivoChem strongly recommends customers to read literature methods/protocols carefully before determining which formulation you should use for in vivo studies, as different compounds have different solubility properties and have to be formulated differently. (Please use freshly prepared in vivo formulations for optimal results.) |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 3.3181 mL | 16.5904 mL | 33.1807 mL | |
| 5 mM | 0.6636 mL | 3.3181 mL | 6.6361 mL | |
| 10 mM | 0.3318 mL | 1.6590 mL | 3.3181 mL |