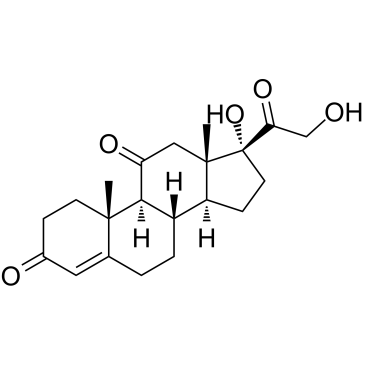
Cortisone is a potent and naturally occurring glucocorticoid with anti-inflammatory activities. It has been used in replacement therapy for adrenal insufficiency and as an anti-inflammatory agent. Cortisone itself is inactive. It is converted in the liver to the active metabolite HYDROCORTISONE.
Physicochemical Properties
| Molecular Formula | C21H28O5 |
| Molecular Weight | 360.45 |
| Exact Mass | 360.193 |
| Elemental Analysis | C, 69.98; H, 7.83; O, 22.19 |
| CAS # | 53-06-5 |
| Related CAS # | Cortisone acetate;50-04-4;Cortisone-d8;Cortisone-13C3;2350278-95-2;Cortisone-d7;1261254-36-7;Cortisone-d2;2687960-86-5 |
| PubChem CID | 222786 |
| Appearance | Typically exists as off-white to light yellow solids at room temperature |
| Density | 1.3±0.1 g/cm3 |
| Boiling Point | 567.8±50.0 °C at 760 mmHg |
| Melting Point | 223-228 °C (dec.)(lit.) |
| Flash Point | 311.2±26.6 °C |
| Vapour Pressure | 0.0±3.5 mmHg at 25°C |
| Index of Refraction | 1.587 |
| LogP | 1.44 |
| Hydrogen Bond Donor Count | 2 |
| Hydrogen Bond Acceptor Count | 5 |
| Rotatable Bond Count | 2 |
| Heavy Atom Count | 26 |
| Complexity | 724 |
| Defined Atom Stereocenter Count | 6 |
| SMILES | C[C@@]1(C2)[C@](C(CO)=O)(O)CC[C@@]1([H])[C@]3([H])CCC4=CC(CC[C@]4(C)[C@@]3([H])C2=O)=O |
| InChi Key | MFYSYFVPBJMHGN-ZPOLXVRWSA-N |
| InChi Code | InChI=1S/C21H28O5/c1-19-7-5-13(23)9-12(19)3-4-14-15-6-8-21(26,17(25)11-22)20(15,2)10-16(24)18(14)19/h9,14-15,18,22,26H,3-8,10-11H2,1-2H3/t14-,15-,18+,19-,20-,21-/m0/s1 |
| Chemical Name | Pregn-4-ene-3,11,20-trione, 17,21-dihydroxy |
| Synonyms | NSC 9703; NSC9703; NSC-9703; 17-Hydroxy-11-dehydrocorticosterone; Kendall's compound E; 53-06-5; Cortisate; Cortistal; Cortivite; Andreson; Cortisal; |
| HS Tariff Code | 2934.99.9001 |
| Storage |
Powder-20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month |
| Shipping Condition | Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs) |
Biological Activity
| Targets | Endogenous Metabolite; immunosuppressant and anti-inflammatory agent; Glucocorticoid-receptor |
| ln Vitro | In peripheral blood mononuclear cells (PBMC), cortisone (2.8-28,000 nM) dose-dependently reduces cortisol-induced apoptosis [1]. |
| ln Vivo |
In rabbits, cortisone (2 mg/kg; intramuscular every other day for two months) decreases tuberculin responses and BCG (Mycobacterium tuberculosis vaccine strain) lesions [2]. The effects of a single dose of cortisone acetate (5 or 10 mg/100 g body weight) on B cells were examined in young chickens. A dose-dependent increase in numbers of circulating B lymphocytes and a change in their Ig-class distribution were followed by parallel increase in splenic plasma cells and serum immunoglobulins. The higher dose of cortisone produced changes in Bmu and Bgamma cells, whereas the lower dose primarily affected Bmu cells. These steroid-induced changes were preceded by lymphocyte depletion in the cortical regions of bursal follicles, and prior bursectomy prevented steroid-induced increases in circulating B lymphocytes and tissue plasma cells. The results suggest that cortisone can induce bursal lymphocytes to migrate from the bursa and to settle subsequently in peripheral lymphoid tissues where they become mature plasma cells[4]. |
| Cell Assay | Glucocorticoids (GCs) have been considered to regulate immune cell systems through induction of apoptosis in thymocytes and mature peripheral-blood lymphocytes. Here we report that apoptosis induced by cortisol in mitogen-activated peripheral-blood mononuclear cells (PBMC) is suppressed by cortisone, an oxidized metabolite of cortisol. Apoptosis in PBMCs is quantified by a cell death ELISA procedure, which can specifically detect fragmented DNA. Cortisol induced PBMC-apoptosis at concentrations more than 10 ng/ml (28 nM) in concanavalin A-stimulated PBMCs and cortisone suppressed this apoptosis at a concentration range of 1-10,000 ng/ml (2.8-28,000 nM) dose-dependently. Prednisone, a synthetic oxidized-GC, also suppressed the apoptosis-inducing effect of cortisol in a dose-dependent manner. Suppression of cortisol-induced apoptosis by cortisone was consistently observed in PBMCs derived from 16 healthy subjects. Examination for inhibitory activities of the steroids against [3H]dexamethasone binding to PBMCs suggested that cortisone can bind cellular GC-receptors (GC-Rs), but the affinity of cortisone to GCRs is 1/30 or less than that of cortisol. The results raised a possible role of cortisone in cortisol-mediated regulation of apoptosis in activated human PBMCs. The counteracting action of cortisone against cortisol-induced apoptosis may take place partially through intervention of GC-receptors (GC-Rs), but may also be due to unknown pathway(s) different from those mediated by cellular GC-Rs[1]. |
| Animal Protocol |
Animal/Disease Models: Male New Zealand white rabbits (2.1-2.4 kg) were injected with BCG six days after the first dose [2] Doses: 2 mg/kg Route of Administration: intramuscularinjection every other day for 2 months Experimental Results: BCG lesions and tuberculosis bacteria were diminished factor reaction. diminished the number of infiltrating mononuclear cells (MN), the number of caseous necrosis and ulcers, and the percentage of β-galactosidase-positive NMs. Rabbits were injected intramuscularly with cortisone acetate (2 mg/kg) on alternate days. Six days after the first injection these rabbits and controls were injected intradermally in multiple sites with BCG (the vaccine strain of tubercle bacillus). Periodically, over the next 2 months, the resulting lesions were measured and surgically biopsied, and the animals were tuberculin-tested. Macrophage activation in the BCG lesions was evaluated histochemically by staining for beta-galactosidase activity. Both BCG lesions (and tuberculin reactions) in the cortisone-treated group were considerably smaller than those in the control group. Cortisone was highly effective in reducing the number of infiltrating mononuclear cells (MN), the amount of caseous necrosis and ulceration, and the percent of NM that were beta-galactosidase-positive. The decreased activation and reduced number of macrophages readily explains the increased susceptibility to tuberculosis found amoung patients receiving glucocorticosteroids. In the BCG lesions, the local decrease in the number and function of leukocytes probably explains the decreased tissue necrosis. Such antiinflammatory effects of corticosteroids may offset, in selected antimicrobial-treated cases, the hormone's detrimental effect on host resistance to infectious agents.[2] |
| Toxicity/Toxicokinetics |
Effects During Pregnancy and Lactation ◉ Summary of Use during Lactation Cortisone is a normal component of breastmilk that passes from the mother's bloodstream into milk and might have a role in intestinal maturation, the intestinal microbiome, growth, body composition or neurodevelopment, but adequate studies are lacking. Concentrations follow a diurnal rhythm, with the highest concentrations in the morning at about 7:00 am and the lowest concentrations in the late afternoon and evening. Cortisone has not been studied in breastmilk after exogenous administration in pharmacologic amounts. Although it is unlikely that dangerous amounts of cortisone would reach the infant, a better studied alternate drug might be preferred. Medium to large doses of corticosteroids given systemically or injected into joints or the breast have been reported to cause temporary reduction of lactation. ◉ Effects in Breastfed Infants None reported with any corticosteroid. ◉ Effects on Lactation and Breastmilk Published information on the effects of cortisone on serum prolactin or on lactation in nursing mothers was not found as of the revision date. Medium to large doses of corticosteroids given systemically or injected into joints or the breast have been reported to cause temporary reduction of lactation. A study of 46 women who delivered an infant before 34 weeks of gestation found that a course of another corticosteroid (betamethasone, 2 intramuscular injections of 11.4 mg of betamethasone 24 hours apart) given between 3 and 9 days before delivery resulted in delayed lactogenesis II and lower average milk volumes during the 10 days after delivery. Milk volume was not affected if the infant was delivered less than 3 days or more than 10 days after the mother received the corticosteroid. An equivalent dosage regimen of cortisone might have the same effect. A study of 87 pregnant women found that betamethasone given as above during pregnancy caused a premature stimulation of lactose secretion during pregnancy. Although the increase was statistically significant, the clinical importance appears to be minimal. An equivalent dosage regimen of cortisone might have the same effect. |
| References |
[1]. Cortisone counteracts apoptosis-inducing effect of cortisol in human peripheral-blood mononuclear cells. Int Immunopharmacol. 2001 Nov;1(12):2109-15. [2]. The effect of cortisone on the accumulation, activation, and necrosis of macrophages in tuberculous lesions. Inflammation. 1978 Jun;3(2):159-76. [3]. In Vivo Antifungal Activity of Monolaurin against Candida albicans Biofilms. Biol Pharm Bull. 2018;41(8):1299-1302. [4]. In vivo effects of cortisone on the B cell line in chickens. J Immunol. 1975 Nov;115(5):1370-4. |
| Additional Infomation |
Cortisone is a C21-steroid that is pregn-4-ene substituted by hydroxy groups at positions 17 and 21 and oxo group at positions 3, 11 and 20. It has a role as a human metabolite and a mouse metabolite. It is a 17alpha-hydroxy steroid, a 21-hydroxy steroid, an 11-oxo steroid, a 20-oxo steroid, a C21-steroid, a 3-oxo-Delta(4) steroid, a primary alpha-hydroxy ketone, a tertiary alpha-hydroxy ketone and a glucocorticoid. It derives from a hydride of a pregnane. A naturally occurring glucocorticoid. It has been used in replacement therapy for adrenal insufficiency and as an anti-inflammatory agent. Cortisone itself is inactive. It is converted in the liver to the active metabolite hydrocortisone. (From Martindale, The Extra Pharmacopoeia, 30th ed, p726) Cortisone is a Corticosteroid. The mechanism of action of cortisone is as a Corticosteroid Hormone Receptor Agonist. Cortisone has been reported in Homo sapiens with data available. Therapeutic Cortisone is a corticosteroid with potent glucocorticoid activity. Therapeutic cortisone is the inactive precursor molecule of the active hormone cortisol, which is the hydroxylation product of cortisone by 11-beta-steroid dehydrogenase. Cortisol increases blood pressure and blood sugar levels, and suppresses the immune system, therefore cortisone is used to treat allergies or inflammation. Cortisone is a steroid hormone synthesized and secreted by the adrenal gland and necessary for life. It is involved with maintaining cardiovascular function, blood glucose balance, regulating the inflammatory response and metabolism of proteins, carbohydrates, and fat. A naturally occurring glucocorticoid that has been used in replacement therapy for ADRENAL INSUFFICIENCY and as an anti-inflammatory agent. Cortisone itself is inactive; it is converted in the liver to the active metabolite HYDROCORTISONE. (From Martindale, The Extra Pharmacopoeia, 30th ed, p726) See also: Cortisone Acetate (active moiety of). |
Solubility Data
| Solubility (In Vitro) | DMSO : ~100 mg/mL (~277.44 mM) |
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 2.5 mg/mL (6.94 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 2.5 mg/mL (6.94 mM) (saturation unknown) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. Solubility in Formulation 3: ≥ 2.5 mg/mL (6.94 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 900 μL of corn oil and mix evenly. (Please use freshly prepared in vivo formulations for optimal results.) |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 2.7743 mL | 13.8715 mL | 27.7431 mL | |
| 5 mM | 0.5549 mL | 2.7743 mL | 5.5486 mL | |
| 10 mM | 0.2774 mL | 1.3872 mL | 2.7743 mL |